Review Article
Volume 2 Issue 3 - 2020
A Review on the Relationship between Nutrition and Health Condition in Humans
Department of Biology, College of Natural and Computational Sciences, Ambo University, Ambo, P.O.Box 19, Ethiopia
*Corresponding Author: Damtew Bekele, Department of Biology, College of Natural and Computational Sciences, Ambo University, Ambo, P.O.Box 19, Ethiopia.
Received: July 28, 2020; Published: August 10, 2020
Abstract
Achieving ecologically sustainable food systems for people is one of the greatest challenges facing our world today. Biomedical scientists could provide public health service and knowledge of basic hygiene and are also placed in support of the production of sustainable, nutritious, ethical and safe food delivered with minimal waste to promote human and environmental health. Good health depends on getting enough to eat. A person who does not eat enough of the foods his body needs becomes thin and weak. Malnutrition in relation to parasitosis causes important child health problems and they are trouble in resisting infections and other illnesses. Also, disability and death from many diseases-especially diarrhea, measles, and tuberculosis-are more frequent in persons who are malnourished. Poor nutrition, with its related illnesses, is responsible for more deaths than any other problem, and is an especially great danger to young children in developing countries. The nutrient intake of developing countries in children and adolescents, therefore, appear to fall below recommended levels. Children and adolescents should be encouraged to eat more nutrients to become healthier. This improvement is notable and represents an important public health issue.
Keywords: Food security; Human health; Children; Good Nutrition; Parasitic infection
Introduction
Food security means that everyone has enough safe and nutritious food all year round to lead an active and healthy life. It also means food is produced and distributed in ways that promote a healthy environment, community self-reliance, and enough good food for every person and community.
The unchecked human population growth in the third world countries increases the chances of transmission from the infested to the non-infested members of the community significantly. The population explosion is one of the major causes of the prevailing environmental degradation. The reduction in the productivity of the land as a result of the degradation of the environment also means malnutrition to the subsistence farming communities.
Projections show that feeding a world population of 9 billion people in 2050 would require raising overall food production by some 70% between 2005–07 and 2050 (FAO, 2009). Despite increases in agricultural production during the past two decades, malnutrition rates have not diminished significantly (Masset et al., 2012). Undernutrition remains a significant problem in many developing countries.
All life forms take in nutrients from food, oxygen from air and energy (the calories stored in food), and they release bodily wastes, exhaled carbon dioxide and energy (heat) to their surroundings. Food security exists when all people, at all times, have physical, social and economic access to sufficient, safe and nutritious food which meets their dietary needs and food preferences for an active and healthy life (FAO, 2016).
As children are most at risk at an age when they are both growing and learning, parasitic infections potentially threatens a child’s overall physical and psychological development and may cause or aggravate malnutrition (Stephension et al., 2000). Malnutrition in many developing countries affects the physical, mental, social wellbeing and child development and it is associated with lower enrollment and poor cognitive functioning among children attending school (Francis et al., 2012). These authors also described that the nutritional status of people infected with helminths is altered through a decline in food intake and an increase in nutrient wastage through blood loss, vomiting or diarrhea. In some underdeveloped regions, they are a major cause of childhood diarrhea and stunting of growth and cause significant economic losses related to human health and to agriculture (Roberts et al., 1994; Guerrant et al., 2002).
Food imports into developing countries increased far faster than into developed countries. While gross food imports into developed countries grew by 45 percent between 1970 and 2001, they grew by 115 percent into developing countries (FAO, 2004).
In 2001-03 there were an estimated 854 million undernourished people worldwide (FAO, 2006). In sub-Saharan Africa high values with almost 25 per cent of the population undernourished, i.e. one in four people (FAO et al., 2015). However, for the developing regions as a whole, the share of undernourished people in the total has decreased from 23.3 percent in 1990–92 to 12.9 percent (FAO et al., 2015).
Economic development in many countries masked widening inequities and growing impoverishment, which often lead to malnutrition, which in turn lowers immune defenses. Economic growth is a key success for reducing undernourishment, but it has to be inclusive and provide opportunities for improving the livelihoods of the poor. Enhancing the productivity and incomes of smallholder family farmers is a key to progress.
Most part of developing countries provide suitable environment for the development of vectors of many insect-borne parasites and geohelminths. The habit of eating raw meat, scarcity of water for domestic use in keeping clean and disposing of human waste are other causes for serious health problems in communities.
Health situation
In the underdeveloped countries, the concept of the quality of life is closely linked to the solution of the urgent problems of poverty: hunger and disease. Farmers could not farm if they are stricken by diseases and students could not come to school if there is hunger. Not only the quality of life but life itself is endangered. The quality of life is therefore considered in an urgent and different sense.
In the underdeveloped countries, the concept of the quality of life is closely linked to the solution of the urgent problems of poverty: hunger and disease. Farmers could not farm if they are stricken by diseases and students could not come to school if there is hunger. Not only the quality of life but life itself is endangered. The quality of life is therefore considered in an urgent and different sense.
People need to be healthy to absorb the nutrients from food. When people are weak from illnesses caused by unsafe water, or from long-term illnesses like malaria or HIV/AIDS, they are less able to produce food for themselves and their communities.
The reduction in food production in developing country such as in Ethiopia as a result of the continuing ecological degradation, the consequent famines, displacements, and civil strife have exacerbated the consequences of infection by human parasites. It can be said in general that the diseases common in developing countries include intestinal diseases, trachoma, veneral diseases, malaria, tuberculosis, nutritional diseases are but a few on a long list that result in excessive mortality and morbidity and a general lowering of physical and mental well-being. However, it is suggested that if health manpower is available it may cope with these inhibitor to economic growth and human well-being.
Low-fat diet reduces the risk for the most prevalent form of cancer (Black et al., 1995). The authors conducted a trial with a 2-year dietary intervention with 101 skin cancer patients who were randomized to either (1) a control group that consumed an average 38% of caloric intake as fat with no changes to dietary habits or (2) a low-fat dietary intervention group that limited their calories from fat to 20% of total caloric intake. Patients were examined every four months over the course of the study. No significant differences in total calories consumed or mean body weight were observed between the control and dietary intervention groups. New cancer occurrence was significantly reduced by 90% in the low-fat intervention group compared with controls.
Experiments indicate that polyunsaturated vegetable oils promote cancer more effectively than do saturated fats (e.g., increase free radicals), whereas total dietary fat correlates more significantly with cancer incidence and mortality in the epidemiologic data (Carroll, 1991). In animals, polyunsaturated fatty acids are readily oxidized to yield free radicals and peroxidates that are toxic to cells and related to tumor development (Odeleye et al., 1990). Omega-3 fatty acids (e.g., fatty fish), a class of polyunsaturated fats, however, decrease the number and size of tumors and increase the time elapsed before tumors appear (Simopoulos, 1991).
As regards the low measures of mid arm circumference, it is reinforced by Castiglia (1996) who stated that mid arm circumference reflects the state of muscle and subcutaneous fat so it is affected in protein energy malnutrition especially the non-edematous.
The study in Cameroon by Gabra and Mbofung (2010) showed that malnutrition and parasitosis are important child health problems and they suggested that lunch meals, nutrition education, sanitation education, and treatment of parasitic infections should be added to the school curriculum of school children.
The role of human nutrition
Human nutrition refers to the provision of essential nutrients necessary to support human life and health. Nutrition is concerned with food and how the body uses it. Food is essential for life, providing the fuel the body needs to function and the building blocks that make up cells, tissues, and organs. Therefore, good nutrition is essential for health and the prevention of diseases. Rather than being filled with nutrients, minerals and healthy fats, many everyday foods are filled with sugar and dangerous fats. Research has linked these ingredients to impatience and even aggression. But a healthy diet will boost your mood and even stave off dark feelings.
Human nutrition refers to the provision of essential nutrients necessary to support human life and health. Nutrition is concerned with food and how the body uses it. Food is essential for life, providing the fuel the body needs to function and the building blocks that make up cells, tissues, and organs. Therefore, good nutrition is essential for health and the prevention of diseases. Rather than being filled with nutrients, minerals and healthy fats, many everyday foods are filled with sugar and dangerous fats. Research has linked these ingredients to impatience and even aggression. But a healthy diet will boost your mood and even stave off dark feelings.
The body requires a certain number of calories simply to carry out its basic metabolic functions such as respiration and maintenance of body temperature. Additional calories are needed to support physical activity, fight infection, and rebuild damaged tissues. However, if a person does not take in enough calories, fat is broken down to provide fuel. Once the fat is consumed or if an individual’s metabolism is disrupted due to illness, lean body mass (muscle and organs) is then used for fuel and raw materials.
Iron and Cognitive Function
Iron deficiency is the single most significant nutrient deficiency, affecting 15% of the world population and causing anemia in 40% to 50% of children (Pollit, 1993). Iron is essential for neurologic activity, including synthesis of dopamine, serotonin, catecholamine, and, possibly, myelin formation (Beard et al., 1993). Iron-deficient children have decreased attentiveness, narrow attention span, and perceptual restrictions (Pollitt, 1993).
Iron deficiency is the single most significant nutrient deficiency, affecting 15% of the world population and causing anemia in 40% to 50% of children (Pollit, 1993). Iron is essential for neurologic activity, including synthesis of dopamine, serotonin, catecholamine, and, possibly, myelin formation (Beard et al., 1993). Iron-deficient children have decreased attentiveness, narrow attention span, and perceptual restrictions (Pollitt, 1993).
Good nutrition for Children
Good nutrition helps for all children to grow physically, gives them energy they need to develop in both body and mind, and protects them from illness (Figure 1). Good nutrition is also important for children living with HIV, as these children need more food to stay healthy than other children their age. Medicines for HIV also work better when children have enough to eat (McCallister et al., 2019).
Good nutrition helps for all children to grow physically, gives them energy they need to develop in both body and mind, and protects them from illness (Figure 1). Good nutrition is also important for children living with HIV, as these children need more food to stay healthy than other children their age. Medicines for HIV also work better when children have enough to eat (McCallister et al., 2019).
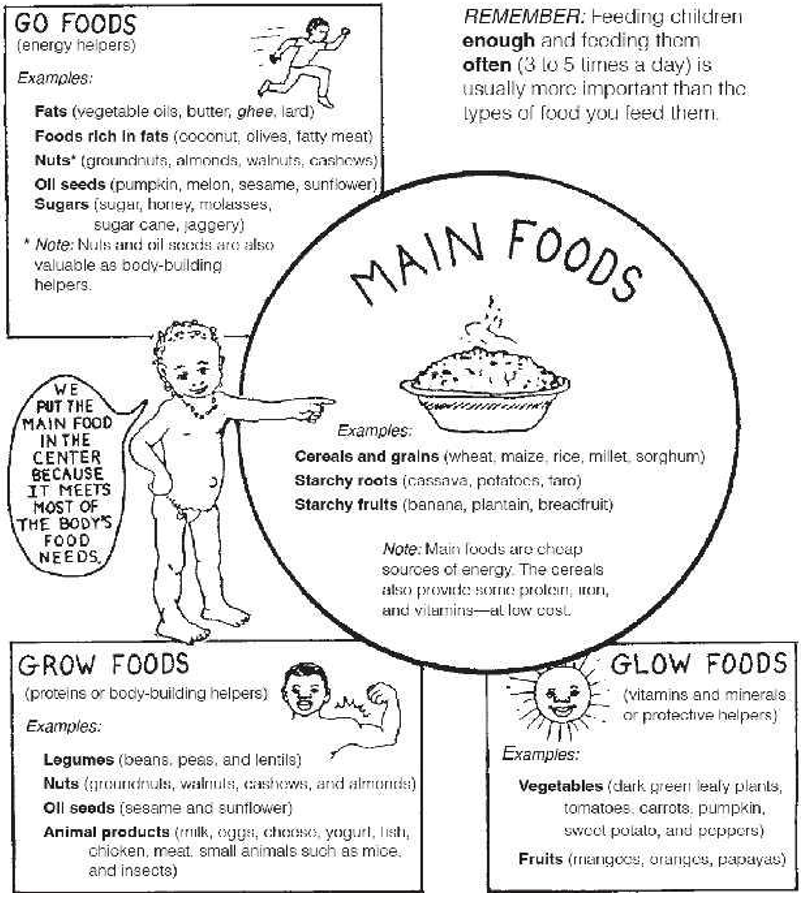
Figure 1: Eating right to stay healthy (adapted from Werner et al., 2015).
Childhood undernutrition remained stubbornly prevalent. The root causes of undernutrition lay in the lack of household economic resources, particularly women’s lack of access to income.
Nutritionists define undernutrition as the inadequate daily intake of diet, measured in calorie intake while malnutrition as imbalance or inadequately in the quality of the diet (Boyd, 1950). If such inadequate calorie intake is allowed to take place over a continuous span of time, the result will be lack of sufficient physical development and less activity on the part of children. For adults, undernutrition could result in reduction of the body weight or physical activity or both.
For the developing regions as a whole, the two indicators of Millennium Development Goals (MDG 1c) the prevalence of undernourishment and the proportion of underweight children under 5 years of age - have both declined (FAO, IFAD and WFP, 2015; IFPRI, 2016). In some regions, including western Africa, south-eastern Asia and South America, undernourishment declined faster than the rate for child underweight, suggesting room for improving the quality of diets, hygiene conditions and access to clean water, particularly for poorer population groups.
Malnutrition causes diarrhea – diarrhea causes malnutrition
For all children, not having enough to eat (malnutrition) and being ill each makes the other worse. When children are ill, they cannot make use of all the nutrition from the food they eat, and they often eat less, making them even weaker and more likely to stay ill or become ill again soon and eventually may lead to death (Figure 2).
For all children, not having enough to eat (malnutrition) and being ill each makes the other worse. When children are ill, they cannot make use of all the nutrition from the food they eat, and they often eat less, making them even weaker and more likely to stay ill or become ill again soon and eventually may lead to death (Figure 2).
Malnutrition lowers resistance to infection, including infection by parasites. As a result, the malnourished people are heavily burdened by a herd of parasites. Malnourished children grow slowly and learn poorly in school, or are too weak to go to school. Moreover, poor nutrition can lead to poor health, which can lead to poor performance at school, and poor schools can lead to unemployment.
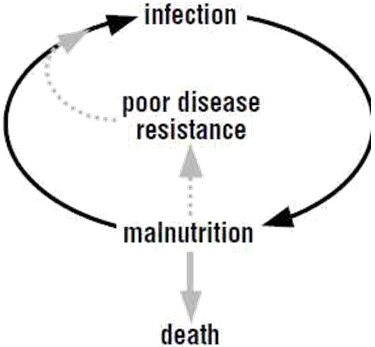
Figure 2: The malnutrition/infection cycle. Good feeding breaks this cycle and saves lives (Adapted from Ashworth, 2002).
Malnutrition harms the whole body, including the gut. The gut, damaged from malnutrition, cannot absorb food well. This results from constant passing of stool which drains the body of nutrients and weakens the child. Therefore malnutrition can be caused by not having enough food, not having enough different kinds of food, or because an illness such as diarrhea makes it hard to absorb food (McCallister et al., 2019). Malnutrition is very dangerous for children with HIV because it makes their weak immune systems even weaker. Thus any child who is malnourished gets other infections much more easily.
Nutrition and Chronic Obstructive Pulmonary Disease (COPD)
Malnutrition is a major concern for individuals with COPD because they have increased energy expenditure, decreased energy intake, and impaired oxygenation (Engelen et al., 1994; Pezza et al., 1994; Palange et al., 1995). These authors described malnutrition as adversely affects exercise tolerance by limiting skeletal and respiratory muscle strength and aerobic capacity, limits surfactant production, reduces cell-mediated immune responses, and reduces protein synthesis.
Malnutrition is a major concern for individuals with COPD because they have increased energy expenditure, decreased energy intake, and impaired oxygenation (Engelen et al., 1994; Pezza et al., 1994; Palange et al., 1995). These authors described malnutrition as adversely affects exercise tolerance by limiting skeletal and respiratory muscle strength and aerobic capacity, limits surfactant production, reduces cell-mediated immune responses, and reduces protein synthesis.
Malabsorption
Various bacterial, viral, fungal, and parasitic infections can interfere with proper nutrition. Several opportunistic infections cause vomiting and diarrhea, which can lead to poor absorption or loss of nutrients. HIV or associated infections can damage the lining of the gastrointestinal tract, which can interfere with absorption of nutrients. Some HIV positive people experience fat malabsorption, which can impair absorption of fat-soluble vitamins.
Various bacterial, viral, fungal, and parasitic infections can interfere with proper nutrition. Several opportunistic infections cause vomiting and diarrhea, which can lead to poor absorption or loss of nutrients. HIV or associated infections can damage the lining of the gastrointestinal tract, which can interfere with absorption of nutrients. Some HIV positive people experience fat malabsorption, which can impair absorption of fat-soluble vitamins.
Avoid unhealthy foods
Local, natural food, the food that our grandparents ate, is better for us than any processed, or junk, food (Conant and Fadem, 2012). Processed foods usually contain a lot of chemicals, salt, and sugar to make them taste good and to addict you to them. They cause health problems such as diabetes, hypertension, heart disease, obesity, headaches, and digestive problems. For example, a 2012 study in Public Health Nutrition (Sánchez-Villegas, et al., 2012) revealed that those who eat junk food are 51 percent likelier to show signs of depression. And the more junk food, the likelier the brain function is impaired. Sugary foods also damage the teeth. In addition, continued increases in the consumption of animal-source foods, as well as energy-rich, nutrient-poor processed foods, has been linked to the rise in overnutrition and associated non-communicable disease such as obesity (Markovic and Natoli, 2009; Wang and Beydoun, 2009). Foods have immense impact on body, so to be healthy and strong, we not only have to eat healthy, nutritious food, but we must also avoid the unhealthy foods.
Local, natural food, the food that our grandparents ate, is better for us than any processed, or junk, food (Conant and Fadem, 2012). Processed foods usually contain a lot of chemicals, salt, and sugar to make them taste good and to addict you to them. They cause health problems such as diabetes, hypertension, heart disease, obesity, headaches, and digestive problems. For example, a 2012 study in Public Health Nutrition (Sánchez-Villegas, et al., 2012) revealed that those who eat junk food are 51 percent likelier to show signs of depression. And the more junk food, the likelier the brain function is impaired. Sugary foods also damage the teeth. In addition, continued increases in the consumption of animal-source foods, as well as energy-rich, nutrient-poor processed foods, has been linked to the rise in overnutrition and associated non-communicable disease such as obesity (Markovic and Natoli, 2009; Wang and Beydoun, 2009). Foods have immense impact on body, so to be healthy and strong, we not only have to eat healthy, nutritious food, but we must also avoid the unhealthy foods.
In developing countries the majority of moderate and severe cases of underweight among children below 2 years are primarily caused by inappropriate weaning practices and a high vulnerability to infectious diseases. One of the infectious diseases most associated with malnutrition among infants is diarrhea, this can often stem from unsafe food. Globalization is often regarded as a danger to food safety since traded food can introduce new hazards and spread contaminated food more widely. There have been some highly publicized cases such as the Cyclospora-related illness from Guatemalan raspberries in the US in 1996 (Unnevehr, 2003).
Nutrition and Parkinson Disease
Unintentional weight loss and declining nutritional status occur commonly in individuals with Parkinson disease (Berry et al., 1995). Explanations for this weight loss include anorexia, difficulty chewing and swallowing, increased time required to complete a meal, reduced sensitivity to smell and taste, depression, increased energy requirements (Levi et al., 1990) because of muscular rigidity and increased involuntary movements, side effects of medications, and decreased intestinal absorption of nutrients (Davis et al., 1996). Nutritional management might include modifying the textures and consistency of foods if chewing and swallowing are problems (Drrieu et al., 1992), offering food supplements and healthful snacks, providing prosthetic devices, and providing assistance with transportation and procurement of food (Berry et al., 1991; Kempster and Wahlqvist, 1994).
Unintentional weight loss and declining nutritional status occur commonly in individuals with Parkinson disease (Berry et al., 1995). Explanations for this weight loss include anorexia, difficulty chewing and swallowing, increased time required to complete a meal, reduced sensitivity to smell and taste, depression, increased energy requirements (Levi et al., 1990) because of muscular rigidity and increased involuntary movements, side effects of medications, and decreased intestinal absorption of nutrients (Davis et al., 1996). Nutritional management might include modifying the textures and consistency of foods if chewing and swallowing are problems (Drrieu et al., 1992), offering food supplements and healthful snacks, providing prosthetic devices, and providing assistance with transportation and procurement of food (Berry et al., 1991; Kempster and Wahlqvist, 1994).
Redistribution of protein may be of benefit, with most of the recommended daily allowance for protein provided in the evening and only 10g of protein in the daytime (Karstaedt and Pincus, 1992; Pare et al., 1992). Benefits within one week were improved daytime mobility at the cost of nighttime rigidity. The other modification is a 5:1 ratio of carbohydrate to protein in a meal that stabilizes the plasma levels of large neutral amino acids and allows for titrating levopoda dosages (Berry et al., 1991). When this dietary modification is helpful, 70% of the people will follow it for longer than one year (Senarath Yapa et al., 1989).
Diet Modifications can Lower Cholesterol
The National Cholesterol Education Program (NCEP, 1991) encourages people with high total cholesterol and low-density lipoprotein (LDL) cholesterol to start with a step I diet that has less than 30% of the total calories coming from fat, 8% to 10% of calories from saturated fat, and less than 300 mg of cholesterol per day. If lipid levels do not decrease after three months, a step II diet is tried in which less than 30% of calories come from total fat, less than 7% from saturated fat, and less than 200 mg from cholesterol (NCEP, 1993). People with high fat baseline diets who lose weight can decrease their cholesterol by 25% with good compliance. Suggestions for lowering fat and saturated fat include: avoiding fats as spreads or for flavoring, avoiding or reducing consumption of meat, using specially manufactured low-fat foods (e.g., fat-free salad dressings), modifying common foods to be lower in fat (e.g., remove skin from chicken), and replacing a high-fat food with its low-fat equivalent (e.g., skin milk instead of whole milk). Children older than two years with high cholesterol levels can follow the NCEP step diet guidelines.
The National Cholesterol Education Program (NCEP, 1991) encourages people with high total cholesterol and low-density lipoprotein (LDL) cholesterol to start with a step I diet that has less than 30% of the total calories coming from fat, 8% to 10% of calories from saturated fat, and less than 300 mg of cholesterol per day. If lipid levels do not decrease after three months, a step II diet is tried in which less than 30% of calories come from total fat, less than 7% from saturated fat, and less than 200 mg from cholesterol (NCEP, 1993). People with high fat baseline diets who lose weight can decrease their cholesterol by 25% with good compliance. Suggestions for lowering fat and saturated fat include: avoiding fats as spreads or for flavoring, avoiding or reducing consumption of meat, using specially manufactured low-fat foods (e.g., fat-free salad dressings), modifying common foods to be lower in fat (e.g., remove skin from chicken), and replacing a high-fat food with its low-fat equivalent (e.g., skin milk instead of whole milk). Children older than two years with high cholesterol levels can follow the NCEP step diet guidelines.
More aggressive diets are also an option for those with high lipid values. These diets contain 10% of total calories from fat, less than 3% from saturated fatty acids (SFAs) and less than 5 mg of cholesterol per day with a minimal amount of animal fat. Labels on food products and nutritional information at fast food restaurants make counting fat grams much easier. Nuts have been shown to lower serum cholesterol levels (Kristal et al., 1992). Walnuts lowered LDL cholesterol by about 16%, and almonds or hazelnuts reduced serum cholesterol by 8% to 10%. Walnuts have a very low ratio of saturated fatty acids to polyunsaturated fatty acids, as well as a high percentage of fat from α-linolenic acid. Including a 1-oz portion of nuts in a low-fat diet should pose no problem while keeping calories under control.
Changing the source of protein may be a method to further lower cholesterol. A meta-analysis found that consuming 31 to 47 g of soybean protein per day significantly decreases serum cholesterol and LDL cholesterol (Lovati et al., 1987). Evidence suggests that soy protein enhances secretion of bile acids and upregulates LDL-receptor activity. Soy protein may be especially helpful in the diets of children diagnosed with familial hypercholesterolemia.
Fat can be replaced with soluble fibers that are known to lower cholesterol levels (Glore et al., 1994). Fibers that have been showing to lower cholesterol and LDL levels include pectins, gums, mucilages, legumes, oats, and carrots. The amount of reduction varies with the source of fiber. Psyllium has been shown to lower LDL levels by 14% in persons with hypercholesterolemia. Two mechanisms have been proposed for the cholesterol-lowering effect: fiber binds the bile acids, which lowers cholesterol to replete the bile acid pool, and bacteria in the colon ferment fiber to compounds (acetate, propionate, and butyrate) that inhibit cholesterol synthesis.
Adding garlic to the diet also may lower cholesterol. Huff (1989) found that 900 mg of powdered garlic (1.5 cloves of garlic) reduced both total cholesterol and LDL cholesterol by about 12%. Fortuantely, cooking does not destroy the allicin (the cardioprotective chemical formed when garlic is crushed) and so the recommendation is simply to include cooked or raw garlic frequently in meals.
Trans-fatty acids are found in many foods, and new data indicate that they may increase a person’s risk of a heart attack (Anderson et al., 1995). The amount of trans-fatty acids in typical margarine ranges from 10% to 30% of total fat and often exceeds 25% in cookies, crackers, pastries, and deep fried foods, such as French fries and doughnuts (Huff, 1989). Researchers have found that trans-fatty acids raise LDL cholesterol, lower the good (high-density lipoprotein [HDL]) and may negatively affect levels of lipoprotein (a), a hereditary risk factor for heart disease.
A person be wary of products that list partially hydrogenated oil on the ingredient list, minimize use of both butter and margarine (choose a fat-free or more liquid version in a tub), cook or bake with olive oil or canola oil, avoid deep fat-fried items, and choose commercially baked items that are either fat free or made with canola or olive oil. What we do not eat may make a difference in our cardiovascular health also. Accumulating data indicate that serum homocysteine concentration is a risk factor for coronary artery disease (Anderson et al., 1995). Acquired homocysteinemia may be the result of vitamin B6, folic acid, or vitamin B12 deficiency. A vitamin B6 deficiency could be a possible risk factor for atherosclerotic disease (Huff, 1989; Anderson et al., 1995). Certainly, including foods high in vitamin B6, such as bananas, broccoli, chicken, dried beans, lean pork, peanut butter, potatoes, tuna fish, and whole wheat bread, can be helpful (Kristal et al., 1992). Epidemiologic evidence that eating no fish at all may be detrimental for the heart is remarkably consistent; however, increasing fish intake beyond one or two servings per week is unlikely to reduce coronary risk substantially in healthy men free of coronary disease.
Nutrition and Hypertension
The effectiveness of weight reduction has been well documented in both mild and severe hypertension. A target for initial weight loss is 4.5 kg. Suggestions for successful weight loss include moderate exercise, moderate calorie restriction, positive self-statements regarding weight loss efforts, self-monitoring activities (food diary, goal setting, early attention to weight gain), and problem solving skills (Mahan and Escott-Stump, 1996).
The effectiveness of weight reduction has been well documented in both mild and severe hypertension. A target for initial weight loss is 4.5 kg. Suggestions for successful weight loss include moderate exercise, moderate calorie restriction, positive self-statements regarding weight loss efforts, self-monitoring activities (food diary, goal setting, early attention to weight gain), and problem solving skills (Mahan and Escott-Stump, 1996).
Some people are salt sensitive including about 30% to 50% of the hypertensive population. Salt sensitivity is defined as a >10 mm Hg decrease in blood pressure by salt depletion after salt loading or more than a 5% increase in blood pressure by salt depletion after restriction of salt (Espinel, 1992). The recommendation for salt intake is no more than 6 g/day, or 2400 mg/day (Espinel, 1992). This can be accomplished by cooking with as little salt as possible; by not adding salt at the table; and by avoiding highly salted and processed foods.
Nutrition and Acute and Chronic Renal Failure
Continuous renal replacement therapy has permitted new approaches to nutrition management with adaptation for individual needs. Calories can be given to meet daily energy expenditure, nitrogen can be given to achieve neutral nitrogen balance, and vitamins and trace elements can be given to meet expected demands (Kierdorf, 1995; Bellomo and Ronco, 1996). Adequate nutritional support promotes renal recovery and may prevent consequences of muscle weakness and immune dysfunction.
Continuous renal replacement therapy has permitted new approaches to nutrition management with adaptation for individual needs. Calories can be given to meet daily energy expenditure, nitrogen can be given to achieve neutral nitrogen balance, and vitamins and trace elements can be given to meet expected demands (Kierdorf, 1995; Bellomo and Ronco, 1996). Adequate nutritional support promotes renal recovery and may prevent consequences of muscle weakness and immune dysfunction.
Indices of malnutrition have also been established for individuals with end-stage renal disease; 20% to 50% are estimated to be malnourished, with morbidity and mortality significantly affected (Ikizler and Hakim, 1996). Catabolism and nutrient loss during dialysis are well documented. Intradialytic parenteral nutrition and use of amino acid dialysate are promising options.
Diverticulitis and Diet
Daily consumption of fiber-enriched foods is recommended for the prevention of diverticula. A high-fiber diet increases fecal bulk, decreases transit time, and eases stool elimination. The recommendation for fiber is 20 to 35 g/day (Bennett and Cerda, 1996). Some examples of high-fiber choices are whole wheat bread and other grain products, baked potato with skin, fresh fruit with skins, raw vegetables, beans, peas, legumes, wheat bran, and brown rice. Side effects may include flatulence, intestinal rumbling, cramps, and diarrhea. A gradual increase in dietary fiber helps to avoid these problems. Other potential problems with an excessively high fiber diet (greater than 40 to 45 gm) might include a decrease in nutrient absorption because of the increased volume of intestinal contents, which in turn decreases the ability of the digestive enzymes to come in contact with the food (Bennett and Cerda, 1996). An increase of water (eight 8-oz glasses) is important so intestinal blockage will not occur (Ozick et al., 1994). For small children and elderly persons a higher-fiber diet increases the volume of food needed to meet energy requirements, and that increase may be difficult to obtain. If the diverticula become inflamed, a low-fiber or low residue (no milk products) diet is required to prevent continued irritation of the inflamed tissue (Ozick et al., 1994).
Daily consumption of fiber-enriched foods is recommended for the prevention of diverticula. A high-fiber diet increases fecal bulk, decreases transit time, and eases stool elimination. The recommendation for fiber is 20 to 35 g/day (Bennett and Cerda, 1996). Some examples of high-fiber choices are whole wheat bread and other grain products, baked potato with skin, fresh fruit with skins, raw vegetables, beans, peas, legumes, wheat bran, and brown rice. Side effects may include flatulence, intestinal rumbling, cramps, and diarrhea. A gradual increase in dietary fiber helps to avoid these problems. Other potential problems with an excessively high fiber diet (greater than 40 to 45 gm) might include a decrease in nutrient absorption because of the increased volume of intestinal contents, which in turn decreases the ability of the digestive enzymes to come in contact with the food (Bennett and Cerda, 1996). An increase of water (eight 8-oz glasses) is important so intestinal blockage will not occur (Ozick et al., 1994). For small children and elderly persons a higher-fiber diet increases the volume of food needed to meet energy requirements, and that increase may be difficult to obtain. If the diverticula become inflamed, a low-fiber or low residue (no milk products) diet is required to prevent continued irritation of the inflamed tissue (Ozick et al., 1994).
A healthy diet depends on biodiversity
Good health depends on eating a variety of foods, such as fruits, vegetables, grains, and wild foods such as berries, fish, and game. When we lose biodiversity, we lose many of the foods we rely on for a healthy diet. Then entire communities are faced with the health problems that come from poor nutrition.
Good health depends on eating a variety of foods, such as fruits, vegetables, grains, and wild foods such as berries, fish, and game. When we lose biodiversity, we lose many of the foods we rely on for a healthy diet. Then entire communities are faced with the health problems that come from poor nutrition.
As a whole, the situation can be regarded as the type of distress which will occur in developing countries with low-developed technology and dependent on unstable weather conditions. The realization of this aspiration demands the tackling of many problems amongst which the control of endoparasitic diseases stands at the forefront. Regarding this health education will help reduce the transmission of parasites that will create a less contaminated environment.
Social protection systems have been critical in fostering progress towards the MDG 1 hunger and poverty targets in a number of developing countries (FAO, IFAD and WFP, 2015). Social protection directly contributes to the reduction of poverty, hunger and malnutrition by promoting income security and access to better nutrition, health care and education.
Balanced diet
A balanced diet is comprised of protein, carbohydrates, fats, fiber, vitamins, and minerals. To obtain a balanced diet it is necessary to eat a wide variety of foods, since a shortage of any of the main classes will result in deficiency diseases. In certain developing countries deficiency diseases are common for three reasons which are shortage of the right kind of food, low incomes (families are often too poor to buy the right kinds of food even if they were available), and superstition and lack of education this include some people may not eat the right foods because they have not been educated in the concepts of a balanced diet. In developing countries including many Ethiopians what they do eat is not a balanced diet. In the face of this major barrier to better health, it does not follow the best way to lower mortality and morbidity.
A balanced diet is comprised of protein, carbohydrates, fats, fiber, vitamins, and minerals. To obtain a balanced diet it is necessary to eat a wide variety of foods, since a shortage of any of the main classes will result in deficiency diseases. In certain developing countries deficiency diseases are common for three reasons which are shortage of the right kind of food, low incomes (families are often too poor to buy the right kinds of food even if they were available), and superstition and lack of education this include some people may not eat the right foods because they have not been educated in the concepts of a balanced diet. In developing countries including many Ethiopians what they do eat is not a balanced diet. In the face of this major barrier to better health, it does not follow the best way to lower mortality and morbidity.
Food contaminated by pesticides, toxic chemicals, germs, or genetically engineered foods, may be available, but will not provide a safe, healthy diet. Also, without a safe cooking space and enough time and fuel to prepare food, people often eat too many processed foods, which can lead to health problems.
Even when food is being produced, it is not used efficiently; considerable energy is lost in fevers of parasitic infections. Heat production in the human body increases about 72 percent for each degree rise in Fahrenheit. A single acute day of fever by malaria requires approximately 500 calories, or an energy demand equivalent to 2 days of hard manual labour (Schmidt and Roberts, 1981). In many developing countries it is estimated that 25-30 percent of the total energy yield from grain production is wasted by fevers caused by parasitic infection and in consumption by parasites (Schmidt and Roberts, 1981). Another cause of energy loss is malabsorption of digested and this is commonplace in parasitic infections. As a sequel of malnutrition and the lowered resistance to infection, opportunistic invasions by helminth larval migrans and protozoans, among others, take place.
Inadequate access to a balanced diet can lead to both undernutrition and overnutrition, resulting in lifelong effects on human health and inefficiencies in food utilization. Food utilization refers to ingestion and digestion of adequate and quality food for maintenance of good health. This means proper biological use of food, requiring a diet that contains sufficient energy and essential nutrients as well as knowledge of food storage, processing, basic nutrition, child care and illness management (Jard et al., 2010).
Food hygiene
Good hygiene when preparing food is always essential but especially when food is being prepared for young children (Ashworth, 2002). Always wash hands with soap and water before handling food. Cooking utensils should be clean. Dry them on a drying rack. Never cough, sneeze or smoke over food that is being prepared for eating. If you are ill, particularly with vomiting or diarrhoea, do not prepare food as you are likely to pass on your infection. Cover cuts and sores on your hands and wear clean clothing.
Good hygiene when preparing food is always essential but especially when food is being prepared for young children (Ashworth, 2002). Always wash hands with soap and water before handling food. Cooking utensils should be clean. Dry them on a drying rack. Never cough, sneeze or smoke over food that is being prepared for eating. If you are ill, particularly with vomiting or diarrhoea, do not prepare food as you are likely to pass on your infection. Cover cuts and sores on your hands and wear clean clothing.
Flies carry disease so food should always be covered. Some food such as milk, eggs, cooked meat, cooked rice and other cereals will spoil more quickly than other kinds of food. Once cooked, food should not be left at normal temperatures for more than two hours. Raw meat and fish, and uncooked vegetables with soil on them, should never come into contact with cooked foods. After handling these foods, wash hands well before handling cooked foods.
Conclusions
Good food is needed for a person to grow well, work hard, and stay healthy. People’s health is weakened if there is no food security and they are vulnerable to any disease. The failure was not that of modern medicine, rather, we were failing to deal with the root causes of disease; lack of food and adequate nutrition, unsafe water, and bad sanitation. Many of the illnesses we were treating could be prevented of we addressed these core problems. Many common sicknesses come from not eating enough. The quality of the farmer’s life is greatly affected by disease. To eliminate the many sources of infections, contagious, nutritional and other diseases, it could surely make a significant contribution to raising the levels of personal hygiene; it could improve eating habits and contribute to communal sanitation. Only by working towards a healthy environment and social justice can we guarantee food security for everyone. Investment in education that is not accompanied by investment in health and nutrition of children is a net loss of a country. Therefore, to prevent diseases improved nutritional status required changes outside the health sector.
Recommendations
There should be altering the conditions of rural life in developing countries by improving agricultural products and controlling debilitating diseases. It also recommended that medical follow-up combined with feeding and teaching basic hygiene. In the process of behavioral change, community participation is essential. Healthy food production and consumption should be a public healthy priority. Preventing and treating diseases like HIV/AIDS, TB, and malaria not only prevents the hunger and malnutrition that go with them, but is important for the entire community’s and food security. Therefore, the promotion of food supplies and proper nutrition are important for prevailing health problems.
There should be altering the conditions of rural life in developing countries by improving agricultural products and controlling debilitating diseases. It also recommended that medical follow-up combined with feeding and teaching basic hygiene. In the process of behavioral change, community participation is essential. Healthy food production and consumption should be a public healthy priority. Preventing and treating diseases like HIV/AIDS, TB, and malaria not only prevents the hunger and malnutrition that go with them, but is important for the entire community’s and food security. Therefore, the promotion of food supplies and proper nutrition are important for prevailing health problems.
References
- Anderson, T.J., Gerhard, M.D., Meredith, I.T., Charbonneau, F., Delagrange, D., Creager, M.A., Selwyn, A.P. and Ganz, P. (1995). Systemic nature of endothelial dysfunction in atherosclerosis. American Journal of Cardiology, 75: 71B-74B.
- Ashworth, A. (2002). Feeding young children. Footsteps, 52: 1-3, London, Tearfund.
- Beard, J.L., Connor, J.R. and Jones, B.C. (1993). Iron in the brain. Nutrition Reviews, 51(6): 157-170.
- Bellomo, R. and Ronco, C. (1996). The nutritional management of acute renal failure in the critically III patients. American Journal of Kidney Disease, 28: S58-S61.
- Bennett, W.G. and Cerda, J.J. (1996). Benefits of dietary fiber. Myth or medicine? Postgraduate Medicine, 99(2): 153-156.
- Berry, P.L., Palarino, M.Y., Michalek, D., Busenbark, K., and Koller, W.C. (1995). Weight changes and body composition in patients with Parkinson’s disease. Journal of American Dietetic Association, 95(5): 979-983.
- Berry, E.M., Growdon, J.H., Wurtman, J.J., Caballero, B. and Wurtman, R.J. (1991). A balanced carbohydrate: protein diet in the management of Parkinson’s disease. Neurology, 41(8): 1295-1297.
- Black, H.S., Thornby, J.I., Wolf Jr. J.E., Goldberg, L.H., Herd, J.A., Rosen, T., Bruce, S., Tschen, J.A., Scott, L.W., Jaax, S., Foreyt, J.P. and Reusser, B. (1995). Evidence that a low-fat diet reduces the occurrence of nonmelanoma skin cancer. International Journal of Cancer, 62(2): 165-169.
- Boyd Orr J. (1950). The food problem. Scientific American, 183: 11-15.
- Carroll, K.K. 1991. Dietary fats and cancer. American Journal of Clinical Nutrition, 53(4): 1064S-1067S
- Castiglia PT. Protein-energy malnutrition (kwashiorkor and marasmus). Journal of Pediatric Health Care 1996, 10: 28-30.
- Conant, J. and Fadem, P. (2012). A community guide to environmental health. Hesperian health guides, Barkeley, California, USA, pp600.
- Davies, K.N., King, D., Billington, D. and Barrett, J.A. (1996). Intestinal permeability and orocaecal transit time in elderly patients with Parkinson’s disease. Postgraduate Medical Journal, 72(845): 164-167.
- Durrieu, G., LLau, M.E., Rascol, O., Senard, J.M., Rascol, A. and Montastruc, J.L. (1992). Parkinson’s disease and weight loss: a study with anthropometric and nutritional assessment. Clinical Autonomic Research, 2(3): 153-157.
- Engelen, M.P., Schols, A.M., Baken, W.C., Wesseling, G.J. and Wouters, E.F. (1994). Nutritional depletion in relation to respiratory and peripheral skeletal muscle function in out-patients with COPD. European Respiratory Journal, 7(10): 1763-1777.
- Espinel, C.H. (1992). The salt step test: its usage in the diagnosis of salt-sensitive hypertension and in the detection of the salt hypertension threshold. Journal of American College of Nutrition, 11(5): 526-531.
- FAO (Food and Agricultural Organization of the United Nations) (2016). Food security statistics. http://www.fao.org/economic/ess/ess-fs/en/ (Accessed 02/09/2016).
- FAO, IFAD and WFP. (2015). The State of Food Insecurity in the World. Meeting the 2015 international hunger targets: taking stock of uneven progress. Rome, FAO, pp62.
- Food and Agriculture Organization of the United Nations (FAO) (2009). Global agriculture towards 2050. High Level Expert Forum: how to feed the world in 2050. FAO, Rome, 2009.
- FAO (2006). The state of food insecurity in the world 2006. Rome
- FAO (2004). The state of agricultural commodity markets (2004). Rome.
- Francis, L., Kirunda, B.E. and Orach, C.G. (2012). Intestinal helminth infections and nutritional status of children attending primary schools in Wakiso District, Central Uganda. International Journal of Environmental Research and Public Health, 9: 2910-2921
- Garba, C.M.G. and Mbofung, C.M.F. (2010). Relationship between malnutrition and parasitic infection among school children in the Adamawa Region of Cameroon. Pakistan Journal of Nutrition, 9(11): 1094-1099.
- Glore, S.R., Van Treeck, D., Knehans, A.W. and Guild, M. (1994). Soluble fiber and serum lipids: a literature review. Journal of American Dietetic Association, 94(4): 425-436.
- Guerrant, R.L., Kosek, M., Moore, S., Lorntz, B., Brantley, R. and Lima, A.A.M. (2002). Magnitude and impact of diarrheal diseases. Archives of Medical Research, 33: 351–355.
- Huff, M.W. (1989). Research horizons in hyperlipidemia and atherosclerosis. Canadian Journal of Cardiology, 5(7): VIII.
- IFPRI (International Food Policy Research Institute). (2016). Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030. Washington, DC: IFPRI.
- Ikizler, T.A., and Hakim, R.M. (1996). Nutrition in end-stage renal disease. Kidney International, 50(2): 343-357.
- Jard, S., Nahas, B. and Baghasa, H. (2010). Food security models. Policy Brief No. 33, Ministry of Agriculture and Agrarian Reform, National Agricultural Policy Center, Syrian Arabic Republic, August 2010, pp: 1-32.
- Karstaedt, P.J. and Pincus, J.H. (1992). Protein redistribution diet remains effective in patients with fluctuating Parkinsonism. Archives of Neurology, 49(2): 149-151.
- Kempster, P.A. and Wahlqvist, M.L. (1994). Dietary factors in management of Parkinson’s disease. Nutrition Reviews, 52: 51-58.
- Kierdorf, H.P. (1995). The nutritional management of acute renal failure in the intensive care unit. New Horizons, 3(4): 699-707.
- Kristal, A.R., White, E., Shattuck, A.L., Curry, S., Anderson, G.L., Fowler, A. and Urban, N. (1992). Long-term maintenance of a low-fat diet: durability of fat-related habits in the women’s health trial. Journal of American Dietetic Association, 92(5): 553-559.
- Levi, S., Cox, M., Lugon, M., Hodkinson, M. and Tomkins, A. (1990). Increased energy expenditure in Parkinson’s disease. British Medical Journal, 301: 1256-1257.
- Lovati, M.R., Manzoni, C., Canavesi, A., Sirtori, M., Vaccarino, V., Marchi, M., Gaddi, G. and Sirtori, C.R. 1987. Soybean protein diet increases low density lipoprotein receptor activity in mononuclear cells from hypercholesterolemic patients. Journal of Clinical Investigation, 80(5): 1498-1502.
- Mahan, L.K. and Escott-Stump, S. (1996). Krause’s food, nutrition, and diet therapy, 9th ed. Philadelphia, Saunders, pp1194.
- Markovic, T.P. and Natoli, S.J. (2009). Paradoxical nutritional deficiency in overweight and obesity: the importance of nutrient density. Medical Journal of Australia, 190: 149–151.
- Masset, E., Haddad, L., Cornelius, A. and Isaza-Castro, J. (2012). Effectiveness of agricultural interventions that aim to improve nutritional status of children: systematic review. British Medical Journal; 344:d8222. doi: 10.1136/bmj.d8222
- McCallister, S., Marinkovich, Z. and Jailer, T. (2019). Helping children live with HIV: Family and community support for vulnerable children. Hesperian health guides, Berkeley, California, USA, pp315.
- National Cholesterol Education Program (NCEP) (1993). Summary of the second report of the National Cholesterol Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel II). Journal of American Association, 269(3): 3015-3023.
- National Cholesterol Education Program (NCEP) (1991). Report of the Expert Panel on population strategies for blood cholesterol reduction: executive summary of National Heart, Lung and Blood Institute, National Institutes of Health. Archives of Internal Medicine, 151(6): 1071-1084.
- Odeleye, O.E., Watson, R.R., Eskelson, C.D. and Mufti, E.S. (1990). Dietary polyunsaturated fatty acid promote peroxidation and its role in the promotion of cancer. Advances in Experimental Medicine and Biology, 283: 789-791.
- Ozick, L.A., Salazar, C.O. and Donelson, S.S. (1994). Pathogenesis, diagnosis, and treatment of diverticular disease of the colon. Gastroenterologist, 2(4): 299-310.
- Palange, P., Forte, S., Felli, A., Galassetti, P., Serra, P. and Carlone, S. 1995. Nutritional state and exercise tolerance in patients with COPD. Chest, 107(5): 1206-1212.
- Pare, S., Barr, S.I. and Ross, S.E. (1992). Effect of daytime protein restriction on nutrient intakes of free-living Parkinson’s disease patients. American Journal of Clinical Nutrition, 55(3): 701-707.
- Pezza, M., Iermano, C. and Tufano, R. (1994). Nutrional support for the patient with chronic obstructive pulmonary disease. Monaldi Archives for Chest Disease, 49: 33-39.
- Pollitt, E. (1993). Iron deficiency and cognitive function. Annual Review of Nutrition, 13: 521-537.
- Roberts, T., Murrell, K.D. and Marks, S. (1994). Economic losses caused by foodborne parasitic diseases. Parasitology Today, 10: 419–423.
- Sánchez-Villegas, A., Toledo, E., de Irala, J., Ruiz-Canela, M., Pla-Vidal, J. and Martínez-González, M.A. (2012). Fast-food and commercial baked goods consumption and the risk of depression. Public Health Nutrition, 15(3), 424–432.
- Schmidt, G.D. and Roberts, L.S. (1981). Foundations of parasitology, 2nd ed. The C.V. Mosby Company. St. Louis. Toronto: London, pp795.
- Senarath Yapa, R.S., Playfer, J.R. and Lye, M. (1989). Anthropometric and nutritional assessment of elderly individuals with Parkinson’s disease. Journal of Clinical Experimental Gerontology, 11: 155-164.
- Simopoulos, A.P. (1991). Omega-3 fatty acids in health and disease and in growth and development. American Journal of Clinical Nutrition, 54(3): 438-463.
- Stephension, L.S., Latham, M.C. and Ottesen, E.A. (2000). Malnutrition and parasitic infections. Parasitology, 121: 532-538.
- Unnevehr, L.J. (2003). Food safety in food security and food trade. 2020 Vision Focus 10. Washington DC: IFPRI.
- Wang, Y. Beydoun, M.A. (2009). Meat consumption is associated with obesity and central obesity among US adults. International Journal of Obesity (Lond), 33: 621–628.
- Werner, D., Thuman, C. and Maxwell, J. (2015). Where there is no doctor: a village health care handbook. Revised Ed Hesperian Health Guides, USA, pp 446.
Citation: Damtew Bekele. (2020). A Review on the Relationship between Nutrition and Health Condition in Humans. Archives of Nutrition and Public Health 2(3).
Copyright: © 2020 Damtew Bekele. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.