Research Article
Volume 2 Issue 5 - 2020
Time Required To Access Electronic Medical Records and the Potential Financial Impact in a Large District General Hospital in England
1FRCSEd, Senior Trauma & Orthopaedic Speciality Surgeon
2MBBS, General Practice Registrar
3FRCS (Tr&Orth), Consultant Trauma & Orthopaedic Surgeon
2MBBS, General Practice Registrar
3FRCS (Tr&Orth), Consultant Trauma & Orthopaedic Surgeon
*Corresponding Author: Haydar Atheer AL HUSSAINY, FRCSEd, Senior Trauma & Orthopaedic Speciality Surgeon, The Department of Trauma & Orthopaedic Surgery, Northampton General Hospital NHS Trust, Northampton, England, The United Kingdom.
Received: November 07, 2020; Published: November 22, 2020
Abstract
Despite the advances in IT systems, computers in hospitals found to be anecdotally slow and inefficient. There is therefore a direct impact on the efficiency of delivering healthcare such as delaying outpatient consultations, interfering with operation theatre flow, and overall disturbing the diagnostic and the therapeutic care provided to patients. The impact of this inefficiency leads to unacceptable time and financial waste within the NHS sector.
In a prospective study, we examine the efficiency of computer terminals in a large district general hospital in United Kingdom by assessing the time required to access electronic medical records (EMR), and estimate the possible financial implications of the time wasted. We also conducted a qualitative survey of staff accessing computer terminals and EMR frequency and experience. One hundred eight computers were recruited in this study in the department of Trauma & Orthopaedics in our institute.
The average time taken for computers to boot up from powered off, and standby to desktop screen in minutes were 4:03 (SD± 2:52), and 2:22 (SD± 1:57) respectively, and that from powered off to accessing x-rays was 5:06 minutes (SD± 3:25). The average daily wasted time (DWT) per worker in our department was 33:22 minutes (SD± 22:20) making the estimated annual money wasted in our department of £543K and that of our hospital and entire NHS of £6 million, and £1.1 billion respectively.
The impact of slow computers in the NHS renders this era of paperless NHS as inefficient in regards to time and finance. Increment in both hardware and software optimisation with improved network bandwidth is imperative to ensure a more efficient future for the NHS.
Keywords: Financial; booting up; Starting up; Computers; Personal computers; Electronic medical records; Electronic health records; National Health Service; NHS.
Abbreviations: CPU- Central Processing Unitl; DWT- daily wasted time; EMR- electronic medical records; Fig -Figure; GB Gigabyte; GHz-Gigahertz; Hdd harddrive; HSCN- Health and Social Care Networking; ID-identification; IE-Internet Explorer; Inc-Incorporation; ITInformation & Technology; K-1000; NHS-National Health Service; PCS-Patient Content Store; RAM-Random Access Memory; SD-Standard Deviation; SSD-solid-state drive; SSO-Single Sign-On; UK-United Kingdom; USA-United States of America; VDI-Virtual Desktop Infrastructure; XR-X-Ray
Introduction
Computers and electronic medical records (EMR) are becoming essential and integral part of healthcare provision all around the world. Such Information & Technology (IT) can improve the quality of care to patients by reducing medical errors, improve communication, and boost efficiency [1-4]. Conversely, when computers struggle, they can bring healthcare providers to a halt [6,7].
Despite the technological advances in hardware and software manufacturing and the astronomical number of calculations supercomputers are able to achieve [7-11]; computers in the National Health Service (NHS) hospitals are still known to be slow [12-14]. According to NHS Digital, more than half of the computers used in NHS hospitals are still operating older versions of windows that are significantly slower than the latest Windows10 version [15,16]. In a recent poll in the United Kingdom (UK) conducted by Medscape, computers took as long as 42 minutes to start up with an average of 7.8 minutes and a median of 5.5 minutes [12]. To remedy such slow performance and according to the Department of Health & Social Care, the UK Government has promised a large lump sum of funds to reduce the staff login times [17].
Slow computers can potentially impact healthcare provision directly by taking professionals away from caring for own patients, delay outpatient clinic consultations, and interfere with the efficiency of operative theatre flow. Similarly, the financial impact for the actual time wasted for computer systems to load up can mount to large sums that are pity to waste [18].
To our knowledge, there has been no peer reviewed English medium publication examining the efficiency of computer systems in practical and real life setup. In orthopaedic surgery over the last decade there has been a paradigm shift in using computer software to interpret fractures, pathology, and plan surgery with significant time spent both in clinics and preoperatively on these systems.
The aim of this study is to ascertain the time required for computers to boot up in our Trauma & Orthopaedic department in a District General Hospital in the UK; as well as estimating the financial implications of the inefficiency on our department, our local institute and on the NHS as a whole.
In addition and to achieve more robust calculation of time consumed for this process of computer start up and logging into the network; we have collected cross-sectional data to reflect staff experience in regards to their daily use of their computer terminals , with emphasis on login attempts per day and applications utilised to access EMR.
Materials and Methods
In a prospective study carried out in the months of January and February of the year 2020, one hundred eight computers allocated to the department of Trauma & Orthopaedics in our institute were included in this study. Inclusion criteria were all desktop and battery operated mobile station computers in wards, theatres, clinics, administration offices, conference and seminar rooms accessed by Trauma & Orthopaedic doctors, nurses, allied health practitioners and administration staff. Laptops and handheld devices were excluded from the study, including tablets, iPads, iPods, and the like. Emergency department & Paediatric ward computers were excluded from the study.
The iPhone timer application (Apple Inc., Cupertino, California, USA) was used to calculate the time to boot up from powered off to login, to enter the user credentials, to get to the desktop screen to access the Internet Explorer (IE) browser (Microsoft©, Redmond, Washington, USA), to use three of the commonly used EMR applications (apps) in our department. For this purpose we used the XRay viewing app Centricity® Universal Zero FootPrint (GE Healthcare, Chicago, Illinois, USA); the patient content store PCS® (Emis Health, Leeds, UK), and the letter dictation apps of Winscribe® (Nuance Communications UK Limited, London, UK).
We recorded the location of each computer, the make, the Random Access Memory (RAM) size in Gigabyte (GB), type of processor, speed of the Central Processing Unit (CPU), type of hard-drive, and the operating system version.
Computers were evaluated by a single assessor at two-months interval and an intra-observer agreement was examined using Bland Altman plot analysis [19]. [Figure 1] Data collected and analysed using Microsoft® Excel® for Mac 2011 version 14, and IBM® SPSS® Statistics V26 software.
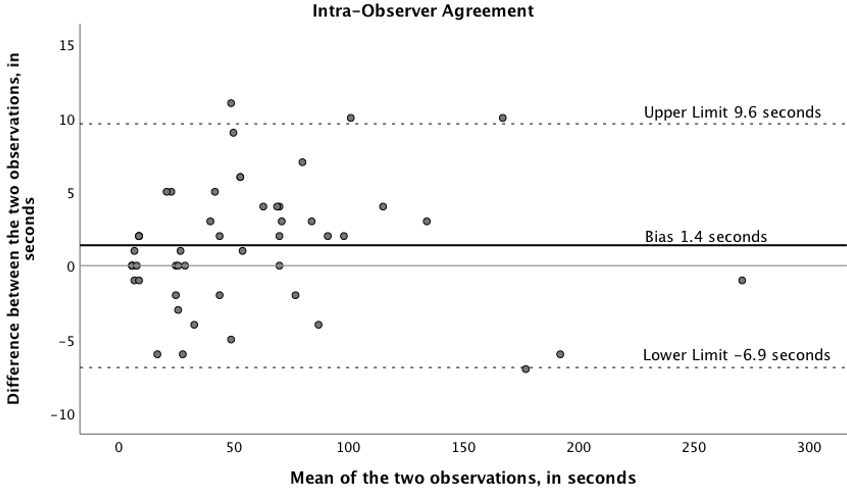
Figure 1: The Bland Altman Agreement plot for the intra-observer agreement analysis showing a bias (the solid black line) of 1.4 seconds (SD± 4.2) away from zero (the solid gray line) difference between the two measurements as assessed two months apart for the same set of fifty computer timing measurements by the same assessor. The dotted lines are the upper and lower 95% confidence interval limits.
One hundred two (94%) out of 108 computers were made by the manufacturer Hewlett-Packard (Hewlett-Packard Company, Palo Alto, California, USA), two were made by Dell (Dell Technologies, Round Rock, Texas, USA), two by Lenovo (Lenovo Group Limited, Beijing, China), one by Venus (Venus Computer Services, Farnham, England, UK), and one by Onyx (Onyx Systems, Inc., Cupertino, California, USA). Ninety-nine computers (92%) had Windows 10 Enterprise installed and nine (8%) had Windows® 7 Professional installed (Microsoft©, Redmond, Washington, USA).
The average central processing unit (CPU) speed was 2.9 GHz (SD± 0.3) (range 1.7-3.5). Forty-nine (45%) computers had Intel© Pentium® architecture, thirty-eight (35%) had Intel© core™ i7, fourteen (13%) had Intel© core™ i5, three for each of Intel© Celeron® and Intel© Xeon®, and one had Intel©, core™ i3 type of CPU processor (Intel©, Santa Clara, California, USA).
The RAM varied from 3-16 Gigabytes (GB), with the majority of 84 (78%) computers having a RAM of 8GB, 19 (18%) of 4GB, and the rest were one computer for each of the 3, 6, 7, 12, and 16GB of RAM equally.
Staff Survey Methods
Two hundred NHS staff in our department of trauma & Orthopaedics were presented with a questionnaire related to their views on the computer performance, availability, number of times they login daily, number of applications used, and worse performing applications.
With a compliance rate of 47%; ninety-three staff members agreed to participate in this survey in March 2020 in our institute. There were 60 females and 33 males. Twenty-eight (30%) were doctors including senior and junior surgical colleagues; twenty-two (24%) were nurses; twenty-five (27%) were allied health practitioners including therapists, and health care assistants; and eighteen (19%) were administration support staff including managers. [Figure 2]
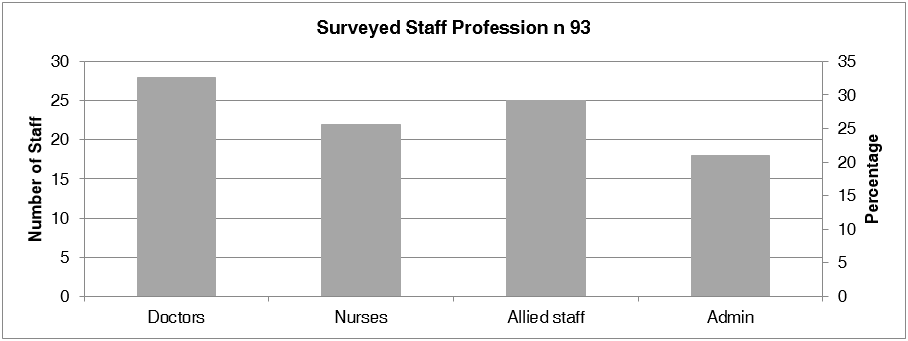
Figure 2: The surveyed staff number and percentage as per profession.
Results
Table 1 details the exact times for every single step of the way from powered off to entering user credentials of username and password, to login into the desktop screen, and to loading all applications. The average time required for computers to boot up from powered off to the desktop screen in minutes: seconds was 4:03 minute (SD± 2:52) (range 1:06-19:56). The fastest was a clinic nursing station computer, and the slowest was computer used by one of the trauma & orthopaedic consultants.
| Powered off to login | Password prompt | Login to desktop | Boot up time | Login from standby | Time per app | |
| Mean | 01:41 | 00:09 | 02:13 | 04:03 | 02:22 | 01:00 |
| SD | 01:22 | 00:04 | 01:57 | 02:52 | 01:57 | 00:44 |
| Min | 00:22 | 00:06 | 00:14 | 01:06 | 00:21 | 00:10 |
| Max | 10:08 | 00:34 | 16:05 | 19:56 | 16:14 | 05:16 |
Table 1: The average times in every step of the way from computers being powered off through booting up, to fully loading an average app. All times shown are in minutes:seconds (mm:ss) format. (SD standard deviation, Min minimum, Max Maximum). Note that the average booting up time of 4:03 minutes equals to 4.05 minutes. This represents the time from powered off until the desktop screen is loaded. n:108
The average time required for computers to resume from standby to the desktop screen was 2:22 minutes (SD± 1:57) (range 0:21-16:14). The fastest was a clinic nursing station computer, and the slowest was a computer used by the same above mentioned consultant.
The average combined time to access the three mostly used EMR software of X-ray viewing, PCS® and letter dictation software (from powered off, one single time, until all three software are fully loaded) was 6:16 minutes (SD± 3:21) (range 2:27-24:03). The fastest was a clinic nursing station computer, and the slowest was used by the same aforementioned consultant. The average time to load one single app from desktop was 01:00 minutes (SD± 00:44) (range 00:10-5:16).
The most commonly used software by orthopaedic surgeons is the XR viewing application, and the time from a powered off state to application start was on average 5:06 minutes (SD± 3:25) (range 1:35-22:06). We found the fastest was the same previously mentioned clinic nursing station computer, and again the slowest was the trauma theatre main computer. Surprisingly, the average time to access the same software from standby status was 3:16 minutes (SD± 2:29) (range 0:42-18:00). The fastest was the same clinic nursing station computer, and the slowest was used by the same consultant mentioned prior. Moreover, the average time required for computers to access the X-Ray viewing software application from the desktop was 1:03 minute (SD± 0:49) (range 0:10-5:16). The fastest was an orthopaedic ward portable computer, and the slowest was the trauma theatre main computer terminal.
Survey results
The average number of times staff needed to login on daily bases were 5.75 times (SD± 4.73) (range 1-20), while the number of applications accessed per user on average was 6.33 apps (SD± 2.49) (range 2-12). We will assume that users might have not accessed all the applications altogether in one single login, therefore and to avoid over-estimating the wasted time calculations; the number of applications has been halved to become 3.17 apps per login. Therefore, the average time required from powered off to having all adjusted average number of apps loaded fully is 10:29 minutes (SD± 6:47) (range 4:06-50:42).
The average number of times staff needed to login on daily bases were 5.75 times (SD± 4.73) (range 1-20), while the number of applications accessed per user on average was 6.33 apps (SD± 2.49) (range 2-12). We will assume that users might have not accessed all the applications altogether in one single login, therefore and to avoid over-estimating the wasted time calculations; the number of applications has been halved to become 3.17 apps per login. Therefore, the average time required from powered off to having all adjusted average number of apps loaded fully is 10:29 minutes (SD± 6:47) (range 4:06-50:42).
Eighteen (19%) of questioned staff rated the computer performance to be ‘good’ or ‘very good’ (one very good, and 17 good), while 32 (34%) thought the speed of computers was fair, and the combined poor and very poor ratings were 43 (47%) out of the 93 surveyed staff. [Figure 3]
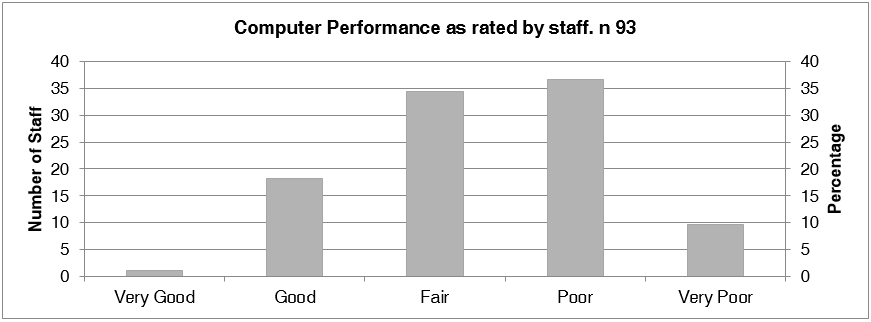
Figure 3: A bar chart showing the computer speed performance in our institute as rated by the surveyed staff. See Text.
Twenty-eight (30%) of the surveyed staff found access to work terminals ‘always easy to find’, 35 (38%) found them ‘most’ of the times, 22 (24%) found computers on ‘sometimes’ bases, and ‘rarely’ in 7 (8%). One did not complete the required questionnaire.
From the 93 surveyed staff, our study found that the applications that were commonly rated as ‘performed badly’ were 165 apps. PCS® n 29 (18%), n 25 (15%) for ICE® (Ice Health systems, Calgary, Canada), n 24 (15%) for Winscribe®, n 19 (12%) for eCamis (Emis Healthcare, Leeds, UK), n 16 (10%) for Symphony® app (Emis Healthcare, Leeds, UK), n 15 (9%) for eDN (Teleologic Ltd, Norwich, UK); n 13 (8%) for the XR viewing app; n 11 (7%) for Microsoft Outlook app (Microsoft©, Redmond, Washington, USA), n 2 (1%) for each of Excel® (Microsoft©, Redmond, Washington, USA), Nexus® (Nexus Health Group, London, UK), and IE apps, and n 1 for each of vitalPac® (System C Healthcare Ltd., Kent, UK), eRoster® (Allocate Software Ltd., London, UK), iBox Dashboards (Intelligent Health Ltd, Reading, UK), Genesis® (Genesis Automation UK Ltd., Bromsgrove, UK), eProcurement® (Advanced Business Software & Solutions, Atlanta, USA), Patchwork® (Patchwork Health, London, UK), CRIS® (Wellbeing Software Group, Mansfield, UK), and The Hive® (Sap, Walldorf, Germany) apps. [Figure 4]
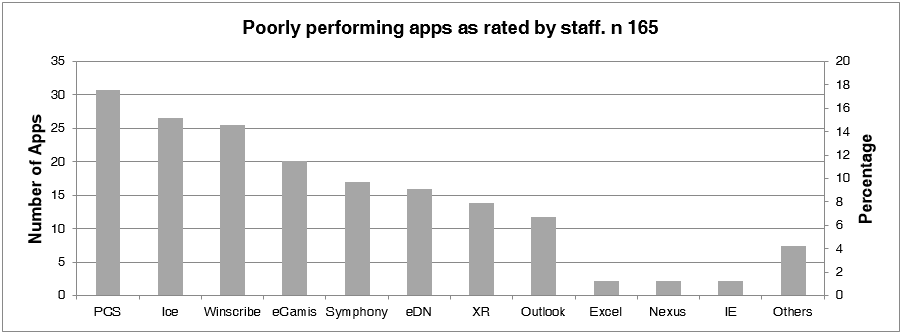
Figure 4: A bar chart demonstrating the worst performing EMR application as rated by the surveyed staff in our department. 165 apps were reported as poor by the 93 surveyed staff.
Financial impact calculations
The NHS provides at 24/7 365 service including weekends, national and local holidays, bank and festive breaks, etc. There is sufficient cover available during sickness and annual leaves to maintain a working service. To avoid financial over estimating the impact of slow computers, we based the calculations on 40 working weeks instead of the 52 weeks of the year, thus excluding twelve weeks to account for the mentioned leaves. We also excluded all weekends (further 80 days), and all bank holidays too (which are usually 8 days every year) leaving 192 days as the effective working days per year for the purpose of this calculation.
The NHS provides at 24/7 365 service including weekends, national and local holidays, bank and festive breaks, etc. There is sufficient cover available during sickness and annual leaves to maintain a working service. To avoid financial over estimating the impact of slow computers, we based the calculations on 40 working weeks instead of the 52 weeks of the year, thus excluding twelve weeks to account for the mentioned leaves. We also excluded all weekends (further 80 days), and all bank holidays too (which are usually 8 days every year) leaving 192 days as the effective working days per year for the purpose of this calculation.
The Daily Wasted Time Calculations
The daily wasted time (DWT) is calculated as [A+B+C (D+B)] where ‘A’ is the average time needed for a user to boot computer up from powered off until the desktop screen. This equates to 4.05 minutes ‘B’ is the time needed for all EMR apps to load (average time per app to load multiplied by the adjusted number of apps). The adjusted number of apps is half the average number of apps as identified in the survey. This equates to 0.99*6.33/2=3.15 minutes. ‘C’ is the remaining number of logins (the average number of logins as identified in the survey minus one, as one login has already been calculated within ‘A’). Therefore C is 5.75-1=4.75 ‘D’ is the average time required from standby to desktop screen as calculated in the study. This equates to 2.36 minutes.
The daily wasted time (DWT) is calculated as [A+B+C (D+B)] where ‘A’ is the average time needed for a user to boot computer up from powered off until the desktop screen. This equates to 4.05 minutes ‘B’ is the time needed for all EMR apps to load (average time per app to load multiplied by the adjusted number of apps). The adjusted number of apps is half the average number of apps as identified in the survey. This equates to 0.99*6.33/2=3.15 minutes. ‘C’ is the remaining number of logins (the average number of logins as identified in the survey minus one, as one login has already been calculated within ‘A’). Therefore C is 5.75-1=4.75 ‘D’ is the average time required from standby to desktop screen as calculated in the study. This equates to 2.36 minutes.
Therefore: DWT=4.05+3.15+4.75*(2.36+3.15) = 33.37 minutes (SD± 22.34) (range 11.2-144.55). This represent the average time wasted per day per worker. In mm:ss format this becomes 33:22 (SD± 22:20) (range 11:12 – 2hrs, 24:33).
The annual financial loss calculations
We have devised a formula to calculate the annual final financial loss for a given institute, hospital, or any healthcare organisation. This is determined by the formula [DWT*aws] where ‘DWT’ represents the Daily Wasted Time, multiplied by ‘a’ (the number of days in a year), multiplied by ‘w’ (the number of workers), multiplied by ‘s’ (the salary wages per minute per worker).
We have devised a formula to calculate the annual final financial loss for a given institute, hospital, or any healthcare organisation. This is determined by the formula [DWT*aws] where ‘DWT’ represents the Daily Wasted Time, multiplied by ‘a’ (the number of days in a year), multiplied by ‘w’ (the number of workers), multiplied by ‘s’ (the salary wages per minute per worker).
Estimated annual financial loss in our Orthopaedic department
In our department, we employed 200 staff at the time of this study, with average salary of £25.3 per hour (£0.42 per minute) as obtained from our local payroll services. The money wasted is estimated to be on average £543K per year in our department, averaging an estimated annual financial loss of £2,701 per worker per year. [Table 2]
In our department, we employed 200 staff at the time of this study, with average salary of £25.3 per hour (£0.42 per minute) as obtained from our local payroll services. The money wasted is estimated to be on average £543K per year in our department, averaging an estimated annual financial loss of £2,701 per worker per year. [Table 2]
| Role | Number of workers | Wages per hour per worker | Wages per minute for all workers | Wasted Money per worker per year | Money Wasted for all workers per year |
| Doctors | 33.6 | 43.6 | 24.4 | 4,652.1 | £156,310 |
| Nurses & Allied Medical Staff | 148.5 | 22.8 | 56.3 | 2,430.1 | £360,892 |
| Administration staff | 18.7 | 12.7 | 4.0 | 1,351.6 | £25,316 |
| Total | 200.8 | 84.7 | £542,518 | ||
| Mean | 25.3 | 0.4* | 2,701.2 |
Table 2: Orthopaedic department money wasted calculations.
Detailed wages calculations as obtained from our local payroll services and the annual wasted money incurred.
*Wages per worker per minute.
Detailed wages calculations as obtained from our local payroll services and the annual wasted money incurred.
*Wages per worker per minute.
Estimated annual financial loss in our hospital
The exact figure of workers that do not use computers is estimated to be 8.7% according to the most recent NHS digital workforce headcount publication. This encompasses hotel & domestic services, estate departments and ambulance staff (NHS Digital, 2020). To avoid overestimating the time wasted even further, the final calculations was based on two thirds of this workforce, assuming that up to one third of the manpower from the total headcount do not regularly use computers, instead of the aforementioned 8.7% figure. Therefore, and after excluding one third of the total headcount; 3200 will remain out of the total of 4800 workers in our hospital. The average salary in our hospital is assumed to be between the national average of £10.07 per hour and the actual £25.3 per hour average salary paid to workers in our department, which makes it £17 per hour per worker. The annual money wasted in our hospital therefore will be in average 6 Million (range 3.4-8.6). [Table 3]
The exact figure of workers that do not use computers is estimated to be 8.7% according to the most recent NHS digital workforce headcount publication. This encompasses hotel & domestic services, estate departments and ambulance staff (NHS Digital, 2020). To avoid overestimating the time wasted even further, the final calculations was based on two thirds of this workforce, assuming that up to one third of the manpower from the total headcount do not regularly use computers, instead of the aforementioned 8.7% figure. Therefore, and after excluding one third of the total headcount; 3200 will remain out of the total of 4800 workers in our hospital. The average salary in our hospital is assumed to be between the national average of £10.07 per hour and the actual £25.3 per hour average salary paid to workers in our department, which makes it £17 per hour per worker. The annual money wasted in our hospital therefore will be in average 6 Million (range 3.4-8.6). [Table 3]
| Wages per hour per worker | Wages per minute per worker | Wasted Money per worker per year | Money Wasted for all workers per year | |
| Best estimate | 10.0 | 0.17 | £1,070 | £3.4 Million |
| Average estimate | 17.7 | 0.29 | £1,886 | £6.0 Million |
| Worst estimate | 25.3 | 0.42 | £2,701 | £8.6 Million |
Table 3: Our hospital estimated annual wasted money.
Detailed calculations of the money wasted in our hospital based on 3200 workers. The best and worst estimates were based on the average income per hour for NHS and that of our Orthopaedic department respectively. See text. Wages are presented in British sterling pounds.
Detailed calculations of the money wasted in our hospital based on 3200 workers. The best and worst estimates were based on the average income per hour for NHS and that of our Orthopaedic department respectively. See text. Wages are presented in British sterling pounds.
Estimated annual financial loss in NHS
Full Fact Charity and NHS Digital indicate that there are roughly 1.5 million people employed by the NHS across the UK [20,21]. Like in the previous local hospital calculations, one million workers are estimated to use computers.
Full Fact Charity and NHS Digital indicate that there are roughly 1.5 million people employed by the NHS across the UK [20,21]. Like in the previous local hospital calculations, one million workers are estimated to use computers.
NHS staff wages range from £7.72-£18.15 with average of £10.07 [22]. The NHS is therefore estimated to waste on slow computers on average £1.1 Billion British Pounds per year (range 0.8-1.9). [Table 4]
| Wages per hour per worker | Wages per minute per worker | Wasted Money per worker per year | Money Wasted for all workers per year | |
| Best estimate | 7.72 | 0.13 | £824 | £0.8 Billion |
| Average estimate | 10.07 | 0.17 | £1,075 | £1.1 Billion |
| Worst estimate | 18.15 | 0.30 | £1,938 | £1.9 Billion |
Table 4: The composition of Satureja khuzistanica essential oils (Khosravinia et al., 2013).
Detailed calculations of the money wasted in NHS in the UK based on one million workers. The best and worst estimates were based on the average income per hour for NHS.
Detailed calculations of the money wasted in NHS in the UK based on one million workers. The best and worst estimates were based on the average income per hour for NHS.
The performance of computers was tested in 5 different groups of users of doctors, clinics, wards, theatres, and administration. Wards’ computers were the fastest with the mean DWT of 32:26 minutes (SD± 15:20), while the poorest in performance were computers used by doctors with mean DWT index of 39.27 minutes (SD± 29.56). Table 5 details the exact number of workstations in each location. There was no statistical significant difference between any of the groups as tested using one-way ANOVA. p>0.9 Computers used by consultant surgeons were slower than those used by junior doctors with DWT of 46:52 minutes (SD± 34:36) and 24:38 minutes (SD± 5:26) respectively.
| Clinics | Admin | Doctors | Wards | Theatres | |
| Mean | 34:53 | 35:25 | 39:27 | 32:26 | 38:25 |
| SD | 19:39 | 20:17 | 29:56 | 15:20 | 38:19 |
| n | 26 | 25 | 16 | 24 | 17 |
Table 5: Location comparison.
This table details the five different computer groups according to their location in our department. SD Standard Deviation, n number of computers. See text.
This table details the five different computer groups according to their location in our department. SD Standard Deviation, n number of computers. See text.
Computer performance Ranking Index vs DWT
Having so many possible variables when assessing the performance of computers, called for a unified benchmarking system to compare performance fairly and more accurately. There are many commercial and open-source benchmarking software in the market, but all need specific software to be installed which is not possible on NHS computers given the potential risk to patients’ data, and to the need for administrative access, which we did not have. Therefore we devised a simple unified benchmark calculated as follows:
Having so many possible variables when assessing the performance of computers, called for a unified benchmarking system to compare performance fairly and more accurately. There are many commercial and open-source benchmarking software in the market, but all need specific software to be installed which is not possible on NHS computers given the potential risk to patients’ data, and to the need for administrative access, which we did not have. Therefore we devised a simple unified benchmark calculated as follows:
WHSPR where ‘W’ is 2.1 or 1 to represents the version of windows being windows10 or windows7 respectively. In our study windows 10 Enterprise performed 2.1 times better than windows 7 professional with means DWT of 31.02 minutes (SD± 17.43) and 65:59 minutes (SD± 48.56) respectively. H is 1.8 or 1 to represents the type of harddrive being ssd, or spinning hdd respectively. From our study, ssd performed 1.8 times better than hdd with means DWT of 33:02 (SD± 20:17), and 61:00 (SD± 38:51) respectively. ‘S’ stands for the absolute CPU speed in GHz as documented in the computer specification accessed from the properties applet.
‘P’ represents the Intel© processor type, and in our study Intel© i7 performed 1.4 faster than Intel© Pentium R with DWT means of 28:26 minutes (SD± 20:39), and 41:40 minutes (SD± 21:30) respectively. Therefore and knowing that Intel© Xeon is progressively faster than i7, which in turn faster than i5, i3, Celeron, and R, we ranked the computers from the slowest R as 1, then 1.2 for Celeron, etc until reaching Xeon that is ranked as 1.6 [23].
Finally ‘R’ represents the Ram, and here we used the absolute Ram number ignoring the GB unit. The mean computer performance-ranking index therefore was calculated to be 89 (SD± 38) (range 9-218). The higher the value, the faster the computer performance is. There was a good inverse linear correlation between the DWT and that of the performance-ranking index with R value of -0.57. This was statistically significant p<0.01 using Pearson’s linear bivariate correlation two tails statistics. (Figure 5)
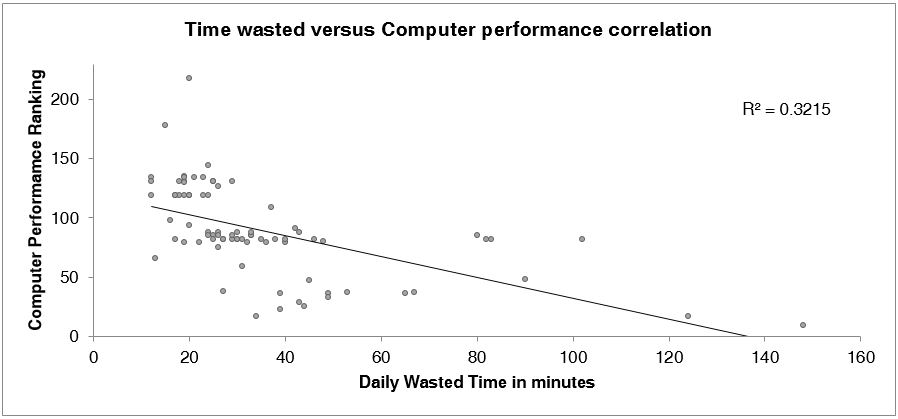
Figure 5: A scatterplot Pearson Linear Correlation graph demonstrates the correlation between the Daily Wasted Time in minutes per worker and the computer performance ranking (the higher the ranking value the better the performance). R is less than one at -0.57. This correlation was statistically significant at p<0.01).
Discussion
Despite significant interest and investment in the NHS since its inception in 1946 [24], we found little published evidence to highlight the changes and increments in the infrastructure of the IT systems utilised in the NHS. The lack of academic scrutiny might have encouraged investigative and political journalists [6,12-14,17], instead, to raise concerns in mainstream media.
We found the average computer speed rather disappointing even from standby, let alone from powered off status. This is collaborated by about half (47%) of the surveyed staff stating that NHS computer performance to be either ‘poor’ or ‘very poor’. This is reflective of the converse, which is found by staff at their homes or via their personal handheld devices and tablets.
Dr Schmidt in 2016 used arbitrary figures to calculate the number of logins and EMRs accessed in each login being five for each respectively [18]. We believe that the DWT devised in this study made the financial impact calculations more accurate and conclusive means. Using such arbitrary figures would have made the DWT 38.34 minutes, instead of our 33.37 minutes. That is five minutes more that would have pushed the final numbers to swell to £623k, £6.9 Million, and £1.2 Billion for the annual wasted money in our department, our hospital, and the entire NHS respectively.
Although PCS® application was found to be the worst performing app out of the 90 apps used in our hospital; reasons suggested for this could be that PCS was one of the most utilised and the most popular app by all staff groups. This very high popularity might cause servers to clog up rendering the app less responsive at times of high activity and demand. We as end-users would still expect such reasons to have been considered by the manufacturer and IT hierarchy prior to going live.
Surprisingly, we found at our hospital that the high priority trauma theatre room computer as one of the worst performing computers despite the heavy traffic and the needs for increased reliability and function. We found it to be the slowest of all computer terminals for loading the XR viewing app from powered off status. We found that this computer still has a spinning hard-drive, a RAM of 4GB, a Celeron® CPU with 2GHz of clock speed, and running Windows® 7 Professional version of operating system. Reasons for such limited upgrades were mainly related to logistical access to the computer hardware as it was fixed and encased by metal enclosure, having the computer housed inside the ultraclean laminar flow theatre room forcing IT staff to having to change into theatre scrubs; and the difficulty accessing busy theatres in daytime working hours compelling IT to send technicians at unsocial afterhours or very early hours in the morning to carryout the upgrades.
Despite having a well equipped IT department and the fundamental reliance on IT, the performance of computers in NHS is surprisingly poor, and reasons we found from this study can be transferred to other hospitals and trusts. Factors such as outdated hardware as 45% of the CPU in our machines were Pentium®, a chip that was introduced by Intel© in 1993 [25], and 3% were Intel© Celeron® microprocessor, a chip that was released in 1999 [26]. It is not a surprise therefore to find that the DWT almost doubling when comparing Intel© core™ i7 and that of Pentium® microprocessors with times of 28:26 minutes (SD± 20:39) and 41:40 minutes (SD± 21:30), respectively. The difference was statistically significant (p<0.003) (one-tailed distribution, Student T Test).
Another reason for slow computers boot up might be related to the type of the local hard-drive harboured in the workstation being a spinning harddisk (hdd) or a solid-state drives (ssd). In our study, such information was available for 104 computers and there were 18 (17%) computers with hdd, and 86 (83%) with ssd computers. The DWT for both were 61:00 (SD± 38:14), and 33:02 (SD± 20:17) for the hdd and the ssd groups respectively. The difference was statistically significant. (p<0.009)
RAM can also affect speed and performance, and in this study we found that the majority 84 (78%) of the computers had a RAM of 8GB, but 22 (21%) were below that. That is 4GB in 19 (18%) computers, and 7,6, and 3GB in one computer each. This does certainly affect the overall speed and performance of NHS computers [27].
Although only nine (8%) computers found to be using windows® 7 Professional operating system in our department; we were surprised still, not just for the known slow and buggy performance, but also for the lack of support from Microsoft corporation, with the extended support ended in January 2020 [28]. Windows® 7 Professional was also found in the aforementioned slowest theatre computer, in three of the four theater computers, and in two of the slowest computers used by consultant surgeons. Having 92% of computers running windows® 10 Enterprise sounds good, but like some believe, Windows® as operating system itself might be the reason behind poor performance and poor speed [29-31].
To simulate a normal daily computer accessing routine, we opted to calculate the time needed to enter credentials of username and password in the actual time wasted calculations. This was in average 00:09 minutes (SD± 00:04) (range 00:06-00:34). The fastest being an HP computer used by one of our advanced nurse practitioners, and the slowest at 34 seconds for the computer used in one of the busiest orthopaedic theatres. The type of the keyboard seems to impact the speed. HP keyboards, for example, are optimised for responsiveness and speed, while those in theatre are slow but optimised for hygiene, cleanliness, and ease to disinfect; for that they are often boxed in and covered by a unibody plastic encasing. On average, the time wasted entering user credentials per day per worker is calculated to be 02:43 minutes (SD± 01:11) (range 01:50-10:20). This includes all logins for all computers per worker per day plus logins for every individual app, which was on average 18.2 times. Each worker would be required to enter credentials therefore 3496 times a year. This mounts to about 702k, 11 Million, and 3.5 Billion logins for our department, our hospital, and the entire NHS respectively.
One of the solutions that are being tested in our institute to reduce the time wasted is to use the Single Sign-On (SSO) technology [32-34], which is based on eliminating the need to enter and re-enter credentials by using the personal identification (ID) security cards that are issued to all workers in the hospital and have imbedded electronic chips programmed to allow staff secure entry to clinical and limited access areas. It is used just like contactless bankcards with much anticipated efficiency in accessing computers and EMRs. We found that using SSO could save just short of three minutes from the DWT of 33.37 as explained earlier to make it 30.38 minutes. Saving £44K, £493K, and £88 Millions for our department, our hospital, and the entire NHS, respectively. These savings are approximately 8% of the wasted time in total as a best estimate. We have over 90 different apps in our institute and it is too premature to tell if the implementation of SSO will be cost effective to the NHS, especially when the average 9 seconds saved per login is still way far from the 4:03 minutes needed to boot up found in our study, or the total of 2:43 minutes potentially saved from 33:22 minutes wasted every day per worker in NHS. It is even farther remote from the 10 seconds booting up time promised by the government [35].
In addition to investing in hardware upgrades, introducing SSO, refining cyber settings, and improving on network bandwidth; other measures and strategies to improve computer performance in NHS could include merging all EMRs into one single platform as in Epic (Epic System Corporation, Verona, Wisconsin, USA); moving to cloud based servers to remove intermediary local servers along with the cost to operate, maintain, upgrade, etc.; optimising and unifying patients records databases [36]; introducing Virtual Desktop Infrastructure (VDI) [37] concept which promises better over all performance than the current discrete real state workstations; and finally move to Health and Social Care Networking (HSCN) which aims to provide safe, reliable, flexible and efficient information sharing between health and social care organisations, who will be able to obtain network connectivity from multiple suppliers, thus improving on network bandwidth even more [38].
Although one may say that waiting for computers to boot up is an unproductive way to spend the time at work and that the time could be utilised for other clinical tasks; we found multiple prompts (such as reinterring credentials, agree to policies, etc) are often needed which in turn keep the clinician at the computer terminal. These prompts were on average approximately 20 per clinical session like that encountered running a follow up orthopaedic clinic for example. Three prompts from powered off to desktop, and on average three prompts per app. These numbers do change periodically to reply to obligatory mass announcement, surveys, upgrade, password expiry prompts, etc.
Conclusions
In summary, we found our Trauma & Orthopaedic department computers to be inefficient and take an excessive amount of time to boot up with DWT (daily wasted time) exceeding 30 minutes per worker with estimated money wasted over £2700 per worker per year. The financial impact of slow computers on the entire NHS is in excess of 1.1 billion British pounds per year.
The proposed DWT calculations and the computer performance benchmark utilised in this study can be used in future research analysis and financial costing impact of health provision.
Acknowledgement
The authors are grateful for the outstanding technichal and IT support of Mr Alfio Al Hussainy who provided insight and expertise that greatly assisted this research study.
The authors are grateful for the outstanding technichal and IT support of Mr Alfio Al Hussainy who provided insight and expertise that greatly assisted this research study.
References
- Chaudhry B, Wang J, Wu S, et al. (2006). Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Annals of internal medicine 144(10): 742-752.
- Main C, Moxham T, Wyatt J, et al. (2010). Computerised decision support systems in order communication for diagnostic, screening or monitoring test ordering: systematic reviews of the effects and cost-effectiveness of systems. Health Technol Assess. 14(48):1-227.
- Kaushal R, Barker KN and Bates DW. (2001). How can information technology improve patient safety and reduce medication errors in children's health care? Archives of pediatrics & adolescent medicine 155(9): 1002-1007.
- Robert Wood Johnson Foundation. (2011). Does Health Information Technology improve quality of care?
- Hoeksma J. (2017). NHS cyberattack may prove to be a valuable wake up call. BMJ 357: j2818.
- Hughes O (2017) WannaCry impact on NHS considerably larger than previously suggested.
- Hockney RW and Jesshope CR. (1988). Parallel Computers 2: architecture, programming and algorithms. CRC Press. Bristol, England; Philadelphia: A. Hilger, 1.1
- Moore GE. (1965). Cramming more components onto integrated circuits. McGraw-Hill New York, NY, USA. 38(8).
- Kurzweil R. (2005). The singularity is near: When humans transcend biology. Penguin. P 70.
- Xin L. (2016). World's fastest supercomputer opens up to users. Physics World 29(8): 11.
- TOP 500 List. (2019). Available at: https://www.top500.org/list/2019/11/?page=1 (accessed June 2020).
- Locke T. (2020). 42 Minute NHS Computer Login Time Tops Medscape UK Slow IT Poll.
- Matthews S. (2019). Britain's top GP reveals it takes her 17 MINUTES to switch on her computer at her NHS practice as Health Secretary Matt Hancock slams her slow tech as being 'totally outrageous' Mail online.
- Winder D. (2019). Login delays are the least of the legacy tech problems facing the NHS. Digital Health.
- Ranger S. (2020). Windows 10 migration struggles: 500,000 NHS computers are still running Windows 7.
- Heath N. (2019). Windows 7 support timebomb: 76% of NHS PCs not on Windows 10 despite looming deadline.
- Hern A. (2020). NHS gets £40m to cut login times on its IT systems.
- Schmidt G. (2016). Health Authority loses millions of dollars to slow computer logins.
- Bland JM and Altman D. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. The lancet 327(8476): 307-310.
- NHS Digital. (2020). NHS Workforce Statistics - January 2020.
- Full Fact. (2017). How many NHS employees are there?
- Pay Scale. (2020). Average Hourly Rate for The National Health Service (NHS) Employees in United Kingdom.
- Covington J. (2019). Xeon vs i7/i5 – What’s the difference?
- Bevan A. (1946). National Health Service Bill, Hansard, HC 5ser. 422, cols: 49–50.
- Alpert D and Avnon D. (1993). Architecture of the Pentium microprocessor. IEEE micro 13(3): 11-21.
- Yew T-G, Li Y-L, Chung C-Y, et al. (1999). Design and performance evaluation of chip capacitors on microprocessor packaging. IEEE 8th Topical Meeting on Electrical Performance of Electronic Packaging (Cat. No. 99TH8412). IEEE, 175-178.
- Life Hacker. (2009). The How-To Geek. Do You Really Need More Than 4GB of RAM?
- Microsoft. (2020). Support for Windows 7 has ended.
- Morgan C. (2019). Windows 10 is the world's most popular desktop operating system, but users still have major complaints about design inconsistencies and buggy updates.
- Hanson M. (2020). Yet another Windows 10 update is causing problems - but Microsoft’s not doing anything about it.).
- Stegner B. (2016). The Most Hated Windows Versions & Why They Were So Bad.
- Wikipedia. (2020). Single Sign-On (SSO).
- The Open Group. (2018). Introduction to Single Sign-On.
- University of Guelph. (2020). SSO Benefits.
- Albert A. (2020). Health Secretary's tech investment promises 'gift of time' to home care workers.
- Helgheim BI, Maia R, Ferreira JC, et al. (2019). Merging data diversity of clinical medical records to improve effectiveness. International journal of environmental research and public health 16(5): 769.
- Rouse M, Madden J. (2017). Desktop virtualization.
- NHS digital. (2020). Health and Social Care Network (HSCN).
Citation: Mr Haydar Atheer AL HUSSAINY, Dr Hasan AL-BAGHDADI and Mr Sami HASSAN. (2020). Time Required To Access Electronic Medical Records and the Potential Financial Impact in a Large District General Hospital in England. Journal of Medical Research and Case Reports 2(5). DOI: 10.5281/zenodo.4285996
Copyright: © 2020 Haydar Atheer AL HUSSAINY. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.