Research Article
Volume 3 Issue 1 - 2021
Nursing Training on Swallowing Screening: Results of a Collaboration Project between Degree Courses in the time of COVID – 19
1Nurse of Complex Structure Internal Medicine, University Health Company Giuliano Isontina, Trieste – Italy
2School of Speech and Language Therapy Trieste – Udine, Department of Medical, Surgical and Health Sciences, University of Trieste, Italy
3Nurse Educator, Degree Course in Nursing, Department of Medical, Surgical and Health Sciences, University of Trieste, Italy
2School of Speech and Language Therapy Trieste – Udine, Department of Medical, Surgical and Health Sciences, University of Trieste, Italy
3Nurse Educator, Degree Course in Nursing, Department of Medical, Surgical and Health Sciences, University of Trieste, Italy
*Corresponding Author: Ana Karina Hinojosa, Nurse Educator – Degree Course in Nursing Department of Medical, Surgical and Health Sciences University of Trieste, Trieste - Italy Strada di Fiume 447, 34149 Trieste – Italy.
Received: February 11, 2021; Published: February 24, 2021
Abstract
Background and Goals: Studies show that Dysphagia is not recognised in half of cases and that specific nurse training is necessary for its identification. The goal of the study was to verify whether university training, aimed at identifying and managing Dysphagia, brought an improvement in students' knowledge in the immediate and 6 months later.
Materials and Methods: 93 students, attending the second year of the Degree in Nursing of Trieste, followed an e-learning laboratory on Dysphagia during the Sars-Cov-2 pandemic. 3 questionnaires at time T0 (pre-training), T1 (after-training) and T2 (6 months later) were administered and compared. Questionnaires T1 and T2 were compared with the achievement of the 4 aims of the study.
Results: 82 students were included. The T0-T1 comparison showed a 3.6 points improvement on average, while the T0-T2 comparison showed equality. The comparison between T1-T2 objectives showed: more than 50% of students reached the 1st target, less than 10% reached the 2nd and 3rd targets and 15% achieved the 4th goal.
Conclusions: Months later, the students didn’t retain the knowledge acquired and the majority of them didn’t achieve the laboratory goals. Results demonstrate the need to combine teaching with laboratory practice or clinical internship.
Keywords: Nursing training; Swallowing screening; Dysphagia
Abbreviations: T0: Time zero; T1: Time one; T2: Time two; SLTT: Speech and Language Therapist teaching Tutor; NE: Nurse Educator
Introduction
Dysphagia can basically be defined as the "abnormal functioning of the swallowing mechanism associated with functional or structural deficits at the oral, pharyngeal or esophageal level". [1]
Studies have shown that older adults may be at risk of Dysphagia due to age related changes called Presbyphagia, i.e. peculiar alterations in the swallowing mechanism. Dysphagia affects up to 30- 40% of people over the age of 65 and is also extremely frequent in neurodegenerative diseases (up to 80%), Stroke (30%), Parkinson's disease (52-82%) and Alzheimer's disease (84%).
Dysphagia reaches the amount of 51% among the elderly admitted to hospital, with an impact on morbidity, length of hospital stay and healthcare costs. [2]
Despite the high prevalence, studies show that Dysphagia is not diagnosed in half of the cases. [3] Therefore, swallowing screening to detect patients with or at risk of Dysphagia is essential to avoid further complications such as aspiration pneumonia, nutritional impairment, dehydration, depression and reduced quality of life. For this reason, Dysphagia significantly affects outcome and is associated with increased morbidity and mortality. [4]
Dysphagia screening should be performed before any oral medications or nutrients are given to the patient. Nurses who are routinely and for long periods of time in close contact with the patient should be familiar with Dysphagia screening protocols [5]; furthermore they should be trained to detect signs and symptoms of Dysphagia and be aware of all signs that indicate a risk of complications such as aspiration in patients with Dysphagia. [6] With this study a specific Dysphagia training, not previously included in the study plan, was introduced in the Degree Course in Nursing of the University of Trieste.
The goal of this study was to implement university nursing student’s knowledge and training in Dysphagia recognition and management, through a collaboration of degree courses.
Materials and Methods
A prospective longitudinal study was conducted by comparing the cognitive and learning tests completed by nursing students at time 0 (pre-training), at T1, immediately after the conclusion of the learning workshop (after-training) and at T2, six months later. The study took place at the Degree Course in Nursing in Trieste in the period between 20 and 27 May and between 23 and 27 October 2020.
The laboratory project was structured on four steps. A total of 93 second year students of the Degree Course in Nursing at the University of Trieste were enrolled to participate to the study.
A Speech and Language Therapist teaching Tutor (SLTT) of the degree course in Speech and Language Therapy and a Nurse Educator (NE) of the degree course in Nursing built two questionnaires used to assess the student basic knowledge and their improvement after the screening laboratory training in the first step of the study.
Three questionnaires were built on Google Forms platform, a Google application that allows the making of online questionnaires. The questionnaires were subsequently administered on-line to all students via a link that allowed them to access to the dedicated form.
The questionnaires were administered at three different times:
At time 0 (T0), ie before the laboratory (pre-training).
At time one (T1), ie immediately after the laboratory (after-training), while the third questionnaire was administered at time two (T2), ie 6 months later.
At time 0 (T0), ie before the laboratory (pre-training).
At time one (T1), ie immediately after the laboratory (after-training), while the third questionnaire was administered at time two (T2), ie 6 months later.
The T0 questionnaire consisted of 11 single correct multiple-choice answer questions divided into 2 sections concerning Dysphagia and the student's internship experiences. This T0 first questionnaire was administered with the purpose of assessing students' basic knowledge and internship experiences.
The T1 and T2 questionnaires consisted of 29 single multiple-choice correct answer questions divided into 4 sections, every single section representing one of the four aims that had to be achieved by the students during the Dysphagia laboratory.
The first section concerned Dysphagia and its characteristics, the second section the identification of patients at risk, the third section the identification of patients needing a swallowing screening test and the fourth section the implementation of the most appropriate nursing interventions to be undertaken after performing the Screening Test. The second part of questionnaire T0 consisted of different questions compared to the questionnaires administered at times T1 and T2. All the questions of the first section of T0, related to Dysphagia, were reported in T1 and T2 with the exception of one question. Furthermore, T1 and T2 contained additional questions, not present in T0.
The three questionnaires were weighted using a 30 points scale and in addition, the last two questionnaires (T1 and T2) were also evaluated on the basis of the achievement of four objectives, equivalent to the 4 sections present in the questionnaires:
1st objective - Knowledge of Dysphagia and its characteristics, 2nd objective - Identification of patients at risk of Dysphagia.
3rd objective - Identification of patients needing a swallowing screening test.
4th objective - Knowledge of the most appropriate nursing interventions to be performed at the end of the screening test. 100% of correct answers were necessary to achieve the goal.
In the second phase of the study, which coincided with the lockdown period following the pandemic caused by the Sars Cov 2 virus, the same students were enrolled to carry out a laboratory on Dysphagia.
The workshop was conducted by a SLTT of the Degree Course in Speech Therapy and by a second- year student of the same Degree Course. The lessons were held electronically through the Microsoft Teams platform.
A team was therefore created for the execution of the laboratory, in which the students accessed via an entry code provided by the teaching tutors of the Degree in Nursing.
The workshop lasted two and a half hours per meeting and was held on four different days, 20-22- 25-27 May, each formed by a group of 20 students.
During the lessons the students were given the anatomical and functional basics of swallowing with hints of anatomy and physiology of the structures involved in the act of swallowing.
The meaning of Dysphagia was then explained to them, presenting its epidemiology, prevalence, the diseases most related to it, the complications, signs and symptoms that accompany it, as well as the risks it entails for those who suffer from it.
In the third step, the Daniels screening test was exposed and illustrated in all its phases, a non- invasive, fast test, which presents minimal risks for the patient, sensitive, specific, validated and which can be administered by the nursing staff.
During the last step of the training laboratory, the correct interventions and their rationale, according to the results of the swallowing screening, were explained and indicated to the students, to guarantee safe nutrition for the patient and to monitor the intake of the meal.
At the end of the laboratory and in preparation for the final test, some possible clinical scenarios were simulated, in which the nurse approaches swallowing screening, asking each individual student questions regarding the resolution of the situation.
The study included:
- The administration of the first questionnaire lasting 10 minutes, immediately before the start of the laboratory at time T0;
- The implementation of university training through the Dysphagia laboratory,
- In the third phase of the study, as soon as the laboratory was completed, ie at time T1, the administration of the second questionnaire lasting 30 minutes,
- In the fourth phase of the study, 6 month later at T2 time, the administration of the third questionnaire, between 23 and 27 October.
- In the fifth phase of the study, the data was analysed.
The study data was reported by Google Forms in an MS Excel spreadsheet. The statistical analysis was carried out using the R version 3.5.0 software.
The collected data were analysed through two comparisons, namely:
- Comparison of marks (expressed in thirties) between T0 and T1 and between T0 and T2;
- Comparison of the objectives achieved in the last two tests (T1 and T2).
The 29 questions present in T1 and T2 have been assigned to a specific objective to be achieved, namely: 1st objective: 3 questions 2nd objective: 11 questions 3rd objective: 11 questions 4th objective: 4 questions
Each correct answer was assigned a value corresponding to 1 point for a total of 29 points and a target overrun rate of 100% was also set.
The continuous variables were described by means of position indices, ie mean and median and represented graphically by means of the Box Plot, while the nominal variables were graphed by means of Bar Graphs. The difference between means was analysed by the Student's t-test for paired data if normally distributed according to the Shapiro-Wilk test. The Wilcoxon's sign for paired variables was chosen in non-normally distributed data. The symmetry in the distribution of the difference in marks with respect to the median of the differences was often approximated, however the sign test was conducted as a verification and confirmation of the Wilcoxon test. For all tests, a significance level was set at = 0.05.
Results
Table Abbreviations: T0: time zero; T1: time one; T2: time two; Min.: minimum; 1st. Qu.: first quartile; 3rd. Qu.: third quartile; Max.: maximum; W: test of Shapiro – Wilk; t: T test right unilateral; df: standard deviation
| Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. | |
| T0 | 8.00 | 17.00 | 21.00 | 20.41 | 25.00 | 30.00 |
Table 1
| Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. | |
| T1 | 16.00 | 22.00 | 25.00 | 24.00 | 26.00 | 29.00 |
Table 2
| Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. | |
| T2 | 8.00 | 19.00 | 22.00 | 21.37 | 24.00 | 29.00 |
Table 3
By means of the Shapiro - Wilk test (table 4) a normal distribution of the differences in the comparison between T0 and T1 and between T0 and T2 was found. The right unilateral Student's t test was therefore performed (table 5) showing that mean at T1 is higher than at T0 of 3.60 points; this difference is statistically significant and consistent with a significant improvement in students’ basic knowledge at the end of the laboratory. The comparison between T0 and T2 shows that the mean at T2 is 0.95 points higher than at T0, therefore this difference is not statistically significant and reflects a partial loss of the knowledge acquired with the laboratory in the following six months.
| W | P – value | |
| T0 – T1 | 0.9827 | 0.3401 |
| T0 – T2 | 0.9805 | 0.2499 |
Table 4: Test of Shapiro – Wilk.
| t | df | P – value | Average of differences | |
| T0 – T1 | 5.4967 | 81 | <0.0001 | 3.5854 |
| T0 – T2 | 1.5334 | 81 | 0.9355 | 0.9512 |
Table 5: Student’s T test right unilateral.
Figure 1 shows the three distributions in comparison using the Box Plot. Both mean and median at T1 and T2 are greater than those at T0, however the difference in these indices between T0 and T2 is very small.

Figure 1: Comparison T0 – T1 – T2.
The objectives achieved in the questionnaires administered at T1 and T2 were also analysed and compared. Tables 6, 7, 8, 9 show the statistical indices of each single objective. In objective 1 and objective 2 median was unchanged over time while mean deviated slightly; in objective 3 both median and mean deviated by 1 point; in objective 4 median differ by 1 point and mean by about 0.7 points.
| Ob. 1 | Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. |
| T1 | 1.000 | 2.000 | 3.000 | 2.585 | 3.000 | 3.000 |
| T2 | 2.000 | 2.000 | 3.000 | 2.524 | 3.000 | 3.000 |
Table 6
| Ob. 2 | Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. |
| T1 | 5.000 | 8.000 | 9.000 | 8.573 | 10.000 | 11.000 |
| T2 | 5.000 | 8.000 | 9.000 | 8.817 | 10.000 | 11.000 |
Table 7
| Ob. 3 | Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. |
| T1 | 5.000 | 8.000 | 9.000 | 8.817 | 10.000 | 11.000 |
| T2 | 4.000 | 7.000 | 8.000 | 7.829 | 9.000 | 11.000 |
Table 8
| Ob. 4 | Min. | 1st Qu. | Median | Mean | 3rd Qu. | Max. |
| T1 | 1.000 | 3.000 | 3.000 | 3.049 | 4.000 | 4.000 |
| T2 | 0.000 | 2.000 | 2.000 | 2.366 | 3.000 | 4.000 |
Table 9
The comparison of the statistical indices between T1 and T2 shows that in both T1 and T2: The 1st goal, i.e. knowledge of Dysphagia and its characteristics, was achieved by at least 50% (median) of the students, as the passing rate was equal to 3.
The 2nd goal, i.e. identification of patients at risk of Dysphagia, and the 3rd goal, i.e. identification of patients needing a swallowing screening test, were achieved by less than 25% (1st quartile) of the students, as the passing rate was 11.
The 4th objective, i.e. knowledge of the most appropriate nursing interventions to be performed at the end of the screening test, was achieved by less than 25% of the students, as the passing rate was equal to 4. In conclusion at least 50% of participants reached the 1st and the 2nd goal, while the 3rd and 4th were achieved by less than 25% of the students.
Figure 2 shows the Box Plots distributions of scores at T1 and T2 both compared for achievement of goal 1 and 2. Medians from T1 to T2 were unchanged.
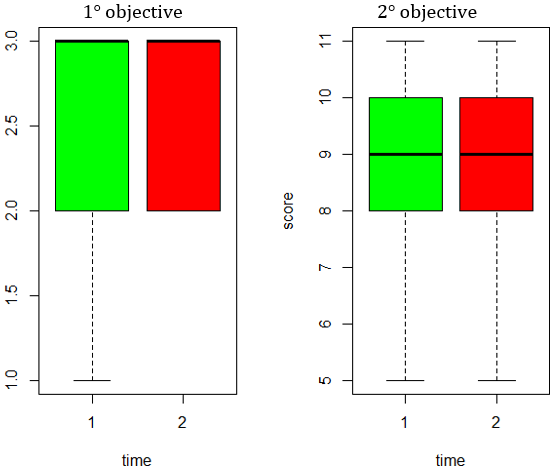
Figure 2: Box Plot: comparison of objectives 1 and 2 between T1 and T2.
Figure 3 shows the Box Plots distributions of scores at T1 and T2 both compared for achievement of goal 3 and 4. Medians at T2 were lower than at T1 for both objectives.
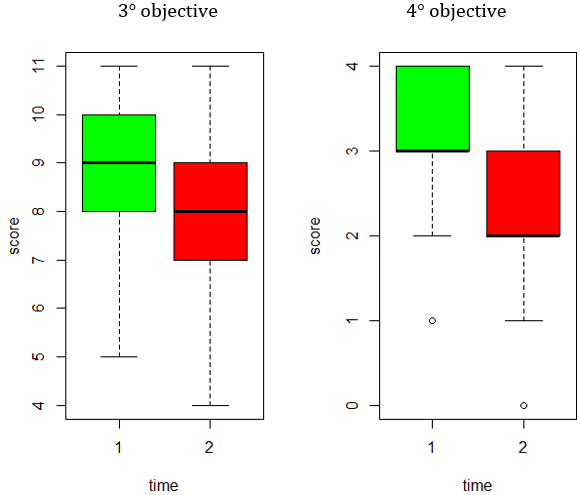
Figure 3: Box Plot: comparison of objectives 3 and 4 between T1 and T2.
Figure 4 shows the comparison between the percentage at T1 and T2 for the achievement of objectives 1 and 2.
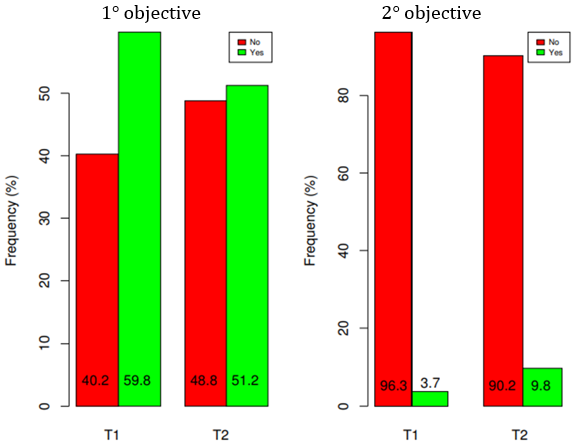
Figure 4: Comparison of objectives 1 and 2 in %.
Figure 5 shows the comparison between the percentage at T1 and T2 for the achievement of objectives 3 and 4.
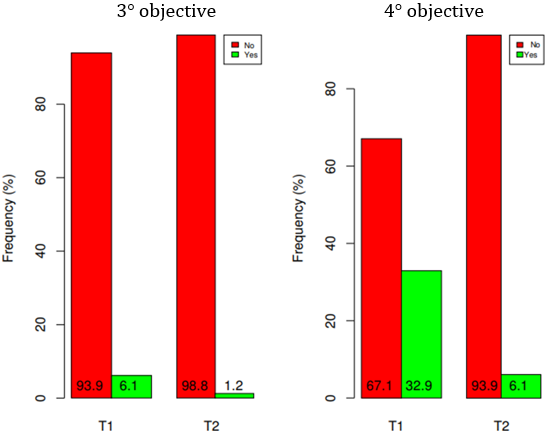
Figure 5: Comparison of objectives 3 and 4 in %.
More than 50% of the students achieved the 1st goal with a 8.6% worsening from T1 to T2, meaning that 8.6% of the students who reached the 1st goal at T1, did not reach it at T2. Less than 10% of students achieved goal 2 with a 6.1% improvement from T1 to T2. Less than 10% of students achieved goal 3 with a 4.9% worsening from T1 to T2. More than 15% of students achieved the 4th goal with a 26.8% worsening from T1 to T2.
Discussion
Dysphagia can basically be defined as the "abnormal swallowing associated with functional or structural deficits at the oral, pharyngeal or esophageal level". [9] There are many and sometimes overlapping causes of Dysphagia manifesting as a mechanical obstruction or a dysfunctional swallowing due to muscles or nerves diseases. [10]
Dysphagia causes serious complications such as malnutrition and/or dehydration, tracheobronchial aspiration, respiratory infections and aspiration pneumonia that can increase morbidity and mortality. [11] Early swallowing screening becomes essential to identify patients at risk, prevent the onset of symptoms and reduce complications. [12]
Therefore the American Speech, Language, Hearing Association recommends that Speech and Language Therapists train Nurses in performing the initial swallowing screening. [5]
The studies also showed that swallowing screening tests should be achieved through a fast and focused training, based on both lectures and practical laboratories by presenting a simple and evidence-based screening tool. [6] The Daniels Test was chosen because of its high sensitivity (93%) [7], easiness to interpret and administer [8], as well as a high inter- and intra-rater agreement. Finally, the Daniels Test was validated by the authors in 2016 as a fast screening test and chosen as a tool to be used for Dysphagia training [7].
The objective of the study was to evaluate the effectiveness of nursing training on the identification and management of Dysphagia patients, aimed at second year students of the Degree in Nursing, through a collaboration between the Degree Course in Nursing and the Degree Course in Speech and Language Therapy.
The training assessment was performed by comparing three questionnaires administered immediately before, immediately after the training and 6 months later.
The comparison of students’ results between T0 and T1 showed an average improvement of 3.6 points; T0 mean was 20.41 out of 30 and 24 out of 30 at T1.
Cichero, Heaton and Bassett in 2009 conducted a similar study. The training evaluation was performed by comparing questionnaires administered in pre- and post-training. The questionnaire consisted of 20 true/false questions divided into 3 sections. Their results showed that the average of the pre - test scores was 17.6 out of 20 and the average of the post - test scores was 18.8 out of 20, with a slight improvement after training. [13]
Our data are in line with that of Cichero, finding a significant improvement after training. We also compared training effects over time and found that the improvement achieved at T1 (i.e. immediately after the laboratory) was lost at T2 (six months later). Our results suggest that further rehearsal of the achieved swallowing testing abilities via practical and simulated training is needed to maintain an adequate level of knowledge over time.
Through the analysis of the achievement of the objectives at T1 and T2 we observed that over 50% of the students reached the 1st goal; less than 10% reached the 2nd and 3rd goal; almost 15% reached the 4th goal. The results from the 1st goal, i.e. knowledge of Dysphagia and its characteristics, probably mean that only theoretical knowledge is required and therefore no further practical simulations are necessary. Consequently, the online laboratory alone was sufficient for the acquisition of these notions. Furthermore, it could be also possible that the lower number of questions related to the 1st objective than to the other goals influenced the greater success of its achievement.
The 2nd, 3rd and 4th training objectives, i.e. identification of patients at risk of Dysphagia, identification of patients needing a swallowing screening test and knowledge of the most appropriate nursing interventions to be performed at the end of the screening test, were not reached by more than 80% of the students.
Although most of the didactic learning can be conducted online, it is nevertheless of fundamental importance that students attend and complete clinical internships in person to meet the requirements necessary for obtaining a degree in Nursing. [14]
Compared to the first, the 3 final objectives probably require the implementation of practical simulations, which were not possible after the establishment of the lockdown in March.
We can therefore state that the primary objective of the study, namely to verify whether the implementation of a university training on the identification and management of Dysphagia patients led to an improvement in students' knowledge, has not been fully achieved, as in immediate post- training, the students have indeed shown an improvement in their knowledge, but after 6 months they almost completely lost it due to the failure to strengthen and consolidate the acquired notions through practical training.
It should be also considered that in the T0 questionnaire 83.3% of the students answered affirmatively to the question "Have you ever had experiences with Dysphagia patients”, but the same 83.3% answered negatively to the question "have you ever conduct a swallowing screening?". Therefore students did never perform a swallowing screening test, while instead during the internship they would have the opportunity to carry it out and at the same time train and strengthen the ability to identify patients at risk, to recognize those to be tested and understanding of the most appropriate nursing interventions to be used in post screening.
Some studies have shown that face-to-face teaching favours theoretical and visual training and that this traditional training is negatively affected in the case of online teaching. In the e-learning modality the student must freely and voluntarily engage in his learning. This model is opposed to the classroom model based on authority and obligation. [5] Morcillo et al [15] highlight the fact that the training of healthcare professionals and professional nurses in particular requires specific professional training, which is developed in the real clinical context. This circumstance cannot be replaced and is indispensable for the development of the know-how of any health professional. [15]
Sullivan et al 16 affirm that clinical experience is perceived as the gold standard of experiential learning in medical-surgical nursing education. It provides students with the opportunity to apply the theoretical knowledge acquired in the classroom thanks to supervised clinical situations. [16]
It can therefore be inferred that the internship could have been useful for the students to strengthen, expand and test the knowledge acquired during the Dysphagia workshop.
For future research it would be appropriate to carry out the study again by unifying the didactic training with practical simulations in order to have a comparison and evaluate whether the addition of clinical practice can improve the training overall.
This study presented some limitations that need to be highlighted. The data presented result from the analysis of 82 students instead of 93, since 11 of them were excluded because either did not answer all the three tests or withdrawn from the degree course.
Another limitation of the study could be associated with the questionnaires administered because they were self-created and not validated, they were not made up of the same questions, leading to a non-homogeneous comparison. Furthermore, the time offered to students for taking the tests may not have been sufficient and some questions may seem ambiguous.
In addition, due to the general lockdown, which occurred following the pandemic caused by Covid 19, the students were unable to carry out practical simulations during internships and received an alternative and very different teaching method, which may have reduced students' concentration and consequently learning.
Conclusion
Nursing training is considered necessary in order to provide the knowledge and information useful to recognize and manage Dysphagia patients. It is essential to consider that the assessment tools cannot be automatically administered by anyone but require a well-planned training program and a high level of attention.
The study shows that, after months, the students have lost most of the knowledge acquired during the online laboratory and that more than 50% have not been able to achieve the set objectives.
It can therefore be stated that the primary objective of the study was not fully achieved, as the students had to carry out distance learning and could not undertake the training internships face to face, consequently these variables could influence negatively on the final outcome which could have instead strengthened and consolidated the knowledge acquired during the workshop on Dysphagia.
The cause of this event can be attributed to the historical period in which the training took place, ie during the lockdown period of the Covid 19 pandemic. Online educational training alone is not sufficient to provide the skills required for a Degree Course in Nursing without accompanying the practical internship necessary for the achievement of the educational objectives of the health profession.
For future research it would be advisable to carry out didactic training, followed and reinforced by practical simulations, in such a way as to allow students to practice what they have learned, be supported by trained personnel and expand their knowledge.
Acknowledgments
The authors are pleased to thank the University of Trieste for allowing the realization of this project.
The authors are pleased to thank the University of Trieste for allowing the realization of this project.
References
- Mandysová, P. et al. (2015). Development of the Brief Bedside Dysphagia Screening Test - Revised: a Cross-Sectional Czech Study. Acta Medica (Hradec Kralove).
- Di Pede, C., Mantovani, M. E., Del Felice, A. & Masiero, S. (2016). Dysphagia in the elderly: focus on rehabilitation strategies. Aging Clin. Exp. Res. 28, 607–617.
- Ellul, J., Barer, D. & Fall, S. (1997). Effects of a coordinated dysphagia management policy on detection and management of swallowing problems in acute stroke, and on functional outcome. J. Neurol. Sci. 84869-1.
- Cecconi, E. & Piero, D. (2012). Dysphagia – Pathophysiology, Diagnosis and Treatment. 30, 86–89.
- Wende N. Fedder. (2017). Review of Evidenced-Based Nursing Protocols for Dysphagia Assessment. Stroke.
- Jiang, J. L., Fu, S. Y., Wang, W. H. & Ma, Y. C. (2016). Validity and reliability of swallowing screening tools used by nurses for dysphagia: A systematic review. Tzu Chi Medical Journal.
- Daniels, S. K., Pathak, S., Rosenbek, J. C., Morgan, R. O. & Anderson, J. A. (2016). Rapid Aspiration Screening for Suspected Stroke: Part 1: Development and Validation. Arch. Phys. Med. Rehabil. 97, 1440–1448.
- Daniels, S. K. et al. (2015). Speech Pathology Reliability for Stroke Swallowing Screening Items. Dysphagia 30, 565–570.
- Mandysová, P., Fusek, J., Tsiou, C. & Plakas, S. (2016). A cross-border educational session promoting nursing dysphagia screening in Greece: A pilot study. Kontakt.
- Wright, D. et al. (2006). Guideline on the medication management of adults with swallowing difficulties. Medicat. Manag. Adults with swallowing difficulties.
- Clavé, P. & Shaker, R. (2015). Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 12, 259–270.
- Martino, R., Pron, G. & Diamant, N. (2000). Screening for oropharyngeal dysphagia in stroke: Insufficient evidence for guidelines. Dysphagia.
- Cichero, J. A., Heaton, S. & Bassett, L. (2009). Triaging dysphagia: Nurse screening for dysphagia in an acute hospital. J. Clin. Nurs.
- Dewart, G., Corcoran, L., Thirsk, L. & Petrovic, K. (2020). Nursing education in a pandemic: Academic challenges in response to COVID-19. Nurse Education Today.
- Ramos-Morcillo, A. J., Leal-Costa, C., Moral-García, J. E. & Ruzafa-Martínez, M. (2020). Experiences of nursing students during the abrupt change from face-to-face to e-learning education during the first month of confinement due to COVID-19 in Spain. Int. J. Environ. Res. Public Health 17, 1–15.
- Sullivan, N. et al. (2019). Emerging Evidence Toward a 2:1 Clinical to Simulation Ratio: A Study Comparing the Traditional Clinical and Simulation Settings. Clin. Simul. Nurs.
Citation: Aurora Laisa, Michelle Passerini and Ana Karina Hinojosa. (2021). “Nursing Training on Swallowing Screening: Results of a Collaboration Project between Degree Courses in the time of COVID – 19”. Journal of Medicine and Surgical Sciences 3.1. DOI: 10.5281/zenodo.4589910
Copyright: © 2021 Ana Karina Hinojosa. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.