Case Report
Volume 7 Issue 1 - 2025
Solitary Fibrous Tumor in the Oral Cavity: A Case Report
MD, Department of Otorhinolaryngology- Head and Neck Surgery, Rizal Medical Center, Pasig Boulevard, Pasig City, 1600, Metro Manila, Philippines
*Corresponding Author: Escientific Publishers, Department of Otorhinolaryngology- Head and Neck Surgery, Rizal Medical Center, Pasig Boulevard, Pasig City, 1600, Metro Manila, Philippines.
Received: March 01, 2025; Published: March 07, 2025
Abstract
This is a case of a 23-year-old male with a 4-year history of gradually enlarging painless mass on the right lateral side of the tongue. There was no associated paresthesia, nor limitation in tongue movement. The physical examination revealed a 2 x 2 cm exophytic, firm, non movable non tender mass on the right lateral tongue. A wedge biopsy of the right lateral tongue mass revealed spindle cell neoplasm. Immunohistochemical staining for TLE1, P40, CD31, desmin, S100 AND Ki67 revealed a low-grade spindle neoplasm most compatible with a solitary fibrous tumor. The patient underwent wide excision of right lateral tongue mass with adequate margins, negative for tumor. Postoperatively, the patient underwent speech therapy. The final histopathology revealed solitary fibrous tumor, which is a rare tumor comprising 2 % of all soft tissue tumors.
Keywords: Solitary fibrous tumor; Spindle neoplasm
Introduction
Solitary fibrous tumors (SFTs) are rare spindle cell neoplasms of mesenchymal origin. They were first documented in 1931 (Klemperer and Rabin 1931), with the neoplasms found arising from pleural cavity. Another case was documented by Stout and Murray in 1942. However, these neoplasms were also found on several sites outside the pleural cavity such as the liver, adrenal gland skin as well as head and neck. Although its incidence in the head and neck is rare, the most common site affected is the oral cavity (Gold 2002).
Over the years, the most population sample documented was done by Ganly et al in 2006 which studied 12 patients from 1990-2004 in New York. To date, there is no published data In the Philippines, on solitary fibrous tumor in the oral cavity. This case aims to document the clinical course of a patient with solitary fibrous tumor in the oral cavity as well as treatment modality and tumor surveillance.
Case
A 23-year-old male presented with a 4-year history of gradually enlarging, painless right lateral tongue mass with no noted inciting event. The patient does not have comorbidities nor family history of cancer. The patient denies history of smoking, alcohol beverage intake and oral sex. On physical examination, there was note of a 2 x 2 cm exophytic, firm, fixed right lateral tongue mass with no involvement of the floor of mouth (Figure 1). There were no palpable cervical lymph nodes.

Figure 1: Right lateral tongue mass on protrusion; A. Anterior view B. Lateral view.
Wedge biopsy of the mass revealed spindle cell neoplasm seen in Figure 2. Immunohistochemical staining revealed positive, strong patchy nuclear staining in tumor cells for STAT 6, and negative, no staining seen for TLE1, P40, CD31, DESMIN, S100. Equivocal to weak moderate patchy staining seen for pancytokeratin and proliferation index up to 5 % in Ki67. The panel revealed findings of a low-grade spindle cell neoplasm most compatible with a solitary fibrous tumor.
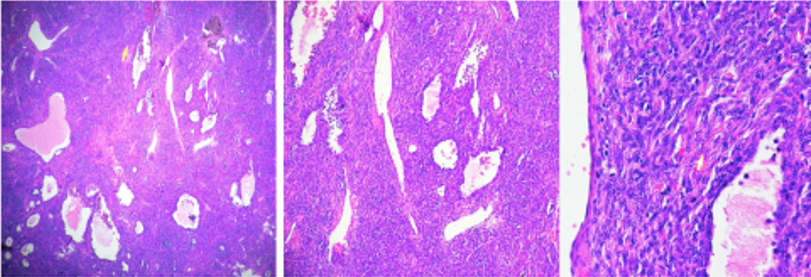
Figure 2: Microscopic view of right lateral tongue mass; A. scanner view B. low power magnification C. High power magnification.
Subsequently, patient underwent wide excision with at least 5 mm margin negative for tumor in all dimensions on frozen section. Primary closure was done as seen in Figure 3.

Figure 3: Primary closure of right lateral tongue A. Anterior view B. Lateral view.
Final histopathology revealed solitary fibrous tumor. Postoperatively, patient underwent rehabilitation therapy for speech.
Discussion
Solitary fibrous tumors (SFT) are spindle cell fibrous and myofibroblastic neoplasms that commonly arise from pleura. They are neoplasms that are accompanied by capillaries (Pitluk and Conn 1979). A rare number are found outside the pleural cavity such as the oral cavity. In the 2005 study by Sakamoto et al, there were only 7 cases of solitary fibrous tumor in the tongue documented. From these cases, the tumors were noted in the fourth to eight decade with the mean age at 58.1. Of these cases, most have been documented in women, in contrast to our case with a male patient presenting with a right lateral tongue mass in the early adulthood.
The patient’s clinical course is similar to previously documented cases. In the study by Ganly et al in 2006, 12 patients with SFTs presented with a gradually enlarging mass of 2 to 60 months duration, with 8 being asymptomatic. These tumors were described as gradually enlarging soft tissue masses that were often found difficult to distinguish from the spectrum of soft tissue tumors such as fibroma, dermatofibrosarcoma and schwannoma. Microscopically, they appear as spindle shaped cells interspersed in haphazard pattern. Thus its diagnosis is difficult to distinguish preoperatively such as in the patient.
Immunohistochemical staining remains the gold standard in establishing the diagnosis. The signature marker of solitary fibrous tumor is the presence of the NAB2- STAT6 fusion that is detected with a STAT6 antibody, a highly sensitive and specific marker. Our patient yielding strong patchy nuclear staining for STAT 6.
Other markers for solitary fibrous tumors of great importance for confirming the diagnosis--- CD34 and Bcl 2. In the study by Sakamoto et al. (2005), CD 34, vimentin, vWf, SMA, desmin, S100, Bcl 2, p53 and Ki67 were entailed. The staining for desmin and S100 were negative in the aforementioned study which were consistent with the patient’s IHC panel. KI 67 proliferation index of < 10% was also seen in the patient with its proliferation index of up to 5%.
Of these markers, presence of CD34 confirms diagnosis of SFTs . In the study by Sakamoto et. Al (2005), CD34 is stipulated as a 110 kDa single-chain transmembrane glycoprotein, which is present on both haematopoietic precursors and capillary endothelial cells. Although most of such tumors are positive for CD34, it is still not specific for SFTs. Certain neoplasms such as neurofibroma, schwannoma, leiomyoma turn out positive for CD34. Thus, exclusion of other neoplasms of mesenchymal origin is needed in establishing the diagnosis of SFTs.
The current treatment modality is surgical excision. Recurrence and metastasis are rare with complete removal of the tumor. (Prado et al 2004).
In the study by De Morais et al (2020), postoperative follow up is recommended for follow up at 45.8 months. Our patient sought follow up with no tumor recurrence. Further solitary fibrous tumors of the oral cavity have better prognosis as compared to extra oral tumors with local invasion, recurrence, intrathoracic dissemination, or distant metastasis documented at 13-23%.
Conclusion
With the patient’s clinical profile, deriving at diagnosis of solitary fibrous tumor is difficult to identify preoperatively. Morphologic and immunohistochemical staining were entailed in establishing the diagnosis. Presence of NAB2-STAT6 fusion detected with a STAT6 antibody is a highly sensitive and specific marker for solitary fibrous tumors. Several markers may also be included in the panel such as CD 34, BCL 2, vimentin and CD 99 but are of low sensitivity and specificity. The current treatment modality is surgical excision. Clinical evaluation for tumor surveillance is recommended, with follow up done up to 45.8 months.
References
- Ganly I, Patel SG, Stambuk HE, et al. Solitary Fibrous Tumors of the Head and Neck:A Clinicopathologic and Radiologic Review. Arch Otolaryngol Head Neck Surg.132(5): 517–525.
- Kei Sakamoto, Toshihiro Sawai, Akira Yamaguchi. (2006). Solitary fibrous tumor of the tongue Oral Oncology Extra, Volume 41, Issue 9, 2005, Pages 222-225
- Pitluk, H. C., & Conn, J. (1979). Hemangiopericytoma. The American Journal of Surgery, 137(3), 413–416.
- Gold JS, Antonescu CR, Hajdu C, et al. (2002). Clinicopathologic correlates of solitary fibrous tumors. Cancer. 94:1057-1068.
- Nardi CEM, Vieira VB, Pfuetzenreiter, Jr EG, Dedivitis RA (2012). Hemangiopericytoma of the tongue. Brazilian Journal of Otorhinolaryngology. 78:136
- De Morais, E., Martins, H., Rodrigues, K., et al. (2020). Clinicopathologic Analysis of Oral and Maxillofacial Solitary Fibrous Tumor: A Systematic Review, American Journal of Clinical Pathology, Volume 154, Issue 1, July 2020, Pages 15– 22.
Citation: Jennifer Anne C. Teves and Samantha S. Castañeda. (2024). Solitary Fibrous Tumor in the Oral Cavity: A Case Report. Journal of Otolaryngology - Head and Neck Diseases 7(1).
Copyright: © 2025 Jennifer Anne C. Teves. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.